China has delayed the return of a crewed mission to the country’s space station over fears that the astronaut’s spacecraft has been struck by space debris. The craft was supposed to return to Earth on 5 November but the China Manned Space Agency says it will now carry out an impact analysis and risk assessment before making any further decisions about when the astonauts will return.
The Shenzhou programme involves taking astronauts to and from China’s Tiangong space station, which was constructed in 2022, for six-month stays.
Shenzhou-20, carrying three crew, launched on 24 April from Jiuquan Satellite Launch Center on board a Long March 2F rocket. Once docked with Tiangong the three-member crew of Shenzhou-19 began handing over control of the station to the crew of Shenzhou-20 before they returned to Earth on 30 April.
The three-member crew of Shenzhou-21 launched on 31 October and underwent the same hand-over process with the crew of Shenzhou-20 before they were set to return to Earth on Wednesday.
Yet pre-operation checks revealed that the craft had been hit by “a small piece of debris” with the location and scale of the damage to Shenzhou-20 having not been released.
If the craft is deemed unsafe following the assessment, it is possible that the crew of Shenzhou-20 will return to Earth aboard Shenzhou-21. Another option is to launch a back-up Shenzhou spacecraft, which remains on stand-by and could be launched within eight days.
Space debris is of increasing concern and this marks the first time that a crewed craft has been delayed due to a potential space debris impact. In 2021, for example, China noted that Tiangong had to perform two emergency avoidance manoeuvres to avoid fragments produced by Starlink satellites that were launched by SpaceX.
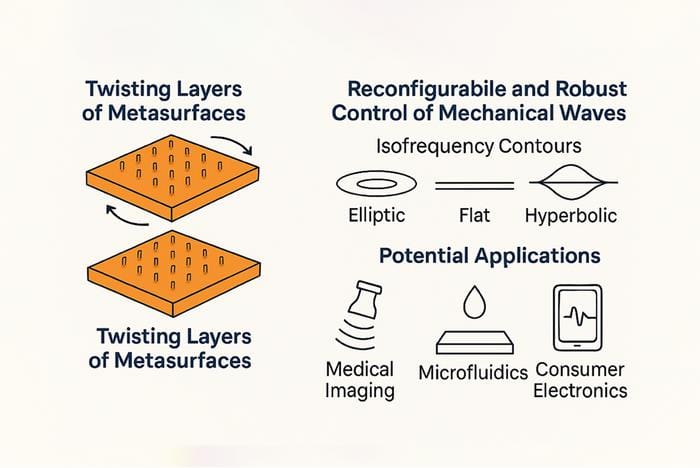
How it works Researchers use twisted surfaces to manipulate mechanical waves, enabling new technologies for imaging, electronics and sensors. (Courtesy: A Alù)
By simply placing two identical elastic metasurfaces atop each other and then rotating them relative to each other, the topology of the elastic waves dispersing through the resulting stacked structure can be changed – from elliptic to hyperbolic. This new control technique, from physicists at the CUNY Advanced Science Research Center in the US, works over a broad frequency range and has been dubbed “twistelastics”. It could allow for advanced reconfigurable phononic devices with potential applications in microelectronics, ultrasound sensing and microfluidics.
The researchers, led by Andrea Alù, say they were inspired by the recent advances in “twistronics” and its “profound impact” on electronic and photonic systems. “Our goal in this work was to explore whether similar twist-induced topological phenomena could be harnessed in elastodynamics in which phonons (vibrations of the crystal lattice) play a central role,” says Alù.
In twistelastics, the rotations between layers of identical, elastic engineered surfaces are used to manipulate how mechanical waves travel through the materials. The new approach, say the CUNY researchers, allows them to reconfigure the behaviour of these waves and precisely control them. “This opens the door to new technologies for sensing, communication and signal processing,” says Alù.
From elliptic to hyperbolic
In their work, the researchers used computer simulations to design metasurfaces patterned with micron-sized pillars. When they stacked one such metasurface atop the other and rotated them at different angles, the resulting combined structure changed the way phonons spread. Indeed, their dispersion topology went from elliptic to hyperbolic.
At a specific rotation angle, known as the “magic angle” (just like in twistronics), the waves become highly focused and begin to travel in one direction. This effect could allow for more efficient signal processing, says Alù, with the signals being easier to control over a wide range of frequencies.
The new twistelastic platform offers broadband, reconfigurable, and robust control over phonon propagation,” he tells Physics World. “This may be highly useful for a wide range of application areas, including surface acoustic wave (SAW) technologies, ultrasound imaging and sensing, microfluidic particle manipulation and on-chip phononic signal processing.
New frontiers
Since the twist-induced transitions are topologically protected, again like in twistronics, the system is resilient to fabrication imperfections, meaning it can be miniaturized and integrated into real-world devices, he adds. “We are part of an exciting science and technology centre called ‘New Frontiers of Sound’, of which I am one of the leaders. The goal of this ambitious centre is to develop new acoustic platforms for the above applications enabling disruptive advances for these technologies.”
Looking ahead, the researchers say they are looking into miniaturizing their metasurface design for integration into microelectromechanical systems (MEMS). They will also be studying multi-layer twistelastic architectures to improve how they can control wave propagation and investigating active tuning mechanisms, such as electromechanical actuation, to dynamically control twist angles. “Adding piezoelectric phenomena for further control and coupling to the electromagnetic waves,” is also on the agenda says Alù.
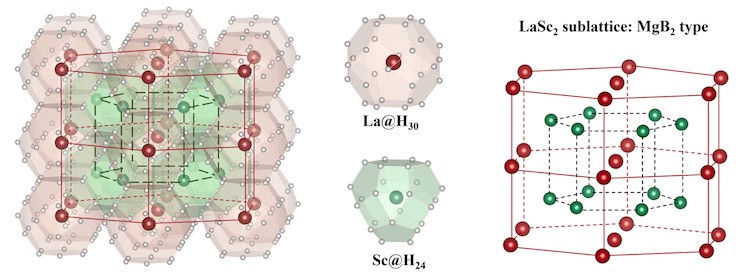
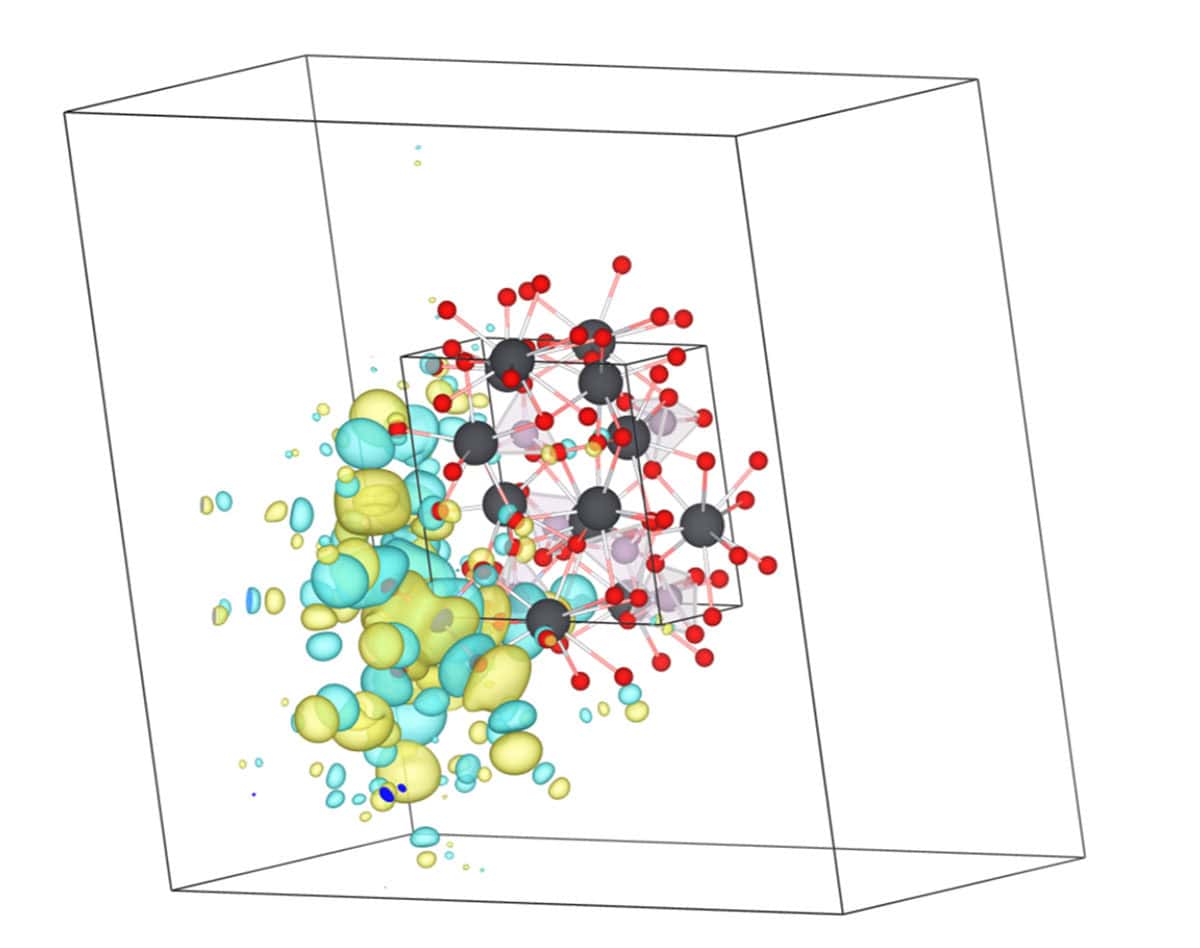
Crystal structure In the new high-Tc superconductor, lanthanum and scandium atoms constitute the MgB2-type sublattice, while the surrounding hydrogen atoms form two types of cage-like configurations. (Courtesy: Guangtao Liu, Jilin University)
Researchers in China claim to have made the first ever room-temperature superconductor by compressing an alloy of lanthanum-scandium (La-Sc) and the hydrogen-rich material ammonia borane (NH3BH3) together at pressures of 250–260 GPa, observing superconductivity with a maximum onset temperature of 298 K. While these high pressures are akin to those at the centre of the Earth, the work marks a milestone in the field of superconductivity, they say.
Superconductors conduct electricity without resistance and many materials do this when cooled below a certain transition temperature, Tc. In most cases this temperature is very low – for example, solid mercury, the first superconductor to be discovered, has a Tc of 4.2 K. Researchers have therefore been looking for superconductors that operate at higher temperatures – perhaps even at room temperature. Such materials could revolutionize a host of application areas, including increasing the efficiency of electrical generators and transmission lines through lossless electricity transmission. They would also greatly simplify technologies such as MRI, for instance, that rely on the generation or detection of magnetic fields.
Researchers made considerable progress towards this goal in the 1980s and 1990s with the discovery of the “high-temperature” copper oxide superconductors, which have Tc values between 30 and 133 K. Fast-forward to 2015 and the maximum known critical temperature rose even higher thanks to the discovery of a sulphide material, H3S, that has a Tc of 203 K when compressed to pressures of 150 GPa.
This result sparked much interest in solid materials containing hydrogen atoms bonded to other elements and in 2019, the record was broken again, this time by lanthanum decahydride (LaH10), which was found to have a Tc of 250–260 K, albeit again at very high pressures. Then in 2021, researchers observed high-temperature superconductivity in the cerium hydrides, CeH9 and CeH10, which are remarkable because they are stable and boast high-temperature superconductivity at lower pressures (about 80 GPa, or 0.8 million atmospheres) than the other so-called “superhydrides”.
Ternary hydrides
In recent years, researchers have started turning their attention to ternary hydrides – substances that comprise three different atomic species rather than just two. Compared with binary hydrides, ternary hydrides are more structurally complex, which may allow them to have higher Tc values. Indeed, Li2MgH16 has been predicted to exhibit “hot” superconductivity with a Tc of 351–473 K under multimegabar pressures and several other high-Tc hydrides, including MBxHy, MBeH8 and Mg2IrH6-7, have been predicted to be stable under comparatively lower pressures.
In the new work, a team led by physicist Yanming Ma of Jilin University, studied LaSc2H24 – a compound that’s made by doping Sc into the well-known La-H binary system. Ma and colleagues had already predicted in theory – using the crystal structure prediction (CALYPSO) method – that this ternary material should feature a hexagonal P6/mmm symmetry. Introducing Sc into the La-H results in the formation of two novel interlinked H24 and H30 hydrogen clathrate “cages” with the H24 surrounding Sc and the H30 surrounding La.
The researchers predicted that these two novel hydrogen frameworks should produce an exceptionally large hydrogen-derived density of states at the Fermi level (the highest energy level that electrons can occupy in a solid at a temperature of absolute zero), as well as enhancing coupling between electrons and phonons (vibrations of the crystal lattice) in the material, leading to an exceptionally high Tc of up to 316 K at high pressure.
To characterize their material, the researchers placed it in a diamond-anvil cell, a device that generates extreme pressures as it squeezes the sample between two tiny, gem-grade crystals of diamond (one of the hardest substances known) while heating it with a laser. In situ X-ray diffraction experiments revealed that the compound crystallizes into a hexagonal structure, in excellent agreement with the predicted P6/mmm LaSc2H24 structure.
A key piece of experimental evidence for superconductivity in the La-Sc-H ternary system, says co-author Guangtao Liu, came from measurements that repeatedly demonstrated the onset of zero electrical resistance below the Tc.
Another significant proof, Liu adds, is that the Tc decreases monotonically with the application of an external magnetic field in a number of independently synthesized samples. “This behaviour is consistent with the conventional theory of superconductivity since an external magnetic field disrupts Cooper pairs – the charge carriers responsible for the zero-resistance state – thereby suppressing superconductivity.”
“These two main observations demonstrate the superconductivity in our synthesized La-Sc-H compound,” he tells Physics World.
Difficult experiments
The experiments were not easy, Liu recalls. The first six months of attempting to synthesize LaSc2H24 below 200 GPa yielded no obvious Tc enhancement. “We then tried higher pressure and above 250 GPa, we had to manually deposit three precursor layers and ensure that four electrodes (for subsequent conductance measurements) were properly connected to the alloy in an extremely small sample chamber, just 10 to 15 µm in size,” he says. “This required hundreds of painstaking repetitions.”
And that was not all: to synthesize the LaSc2H24, the researchers had to prepare the correct molar ratios of a precursor alloy. The Sc and La elements cannot form a solid solution because of their different atomic radii, so using a normal melting method makes it hard to control this ratio. “After about a year of continuous investigations, we finally used the magnetron sputtering method to obtain films of LaSc2H24 with the molar ratios we wanted,” Liu explains. “During the entire process, most of our experiments failed and we ended up damaging at least 70 pairs of diamonds.”
Sven Friedemann of the University of Bristol, who was not involved in this work, says that the study is “an important step forward” for the field of superconductivity with a new record transition temperature of 295 K. “The new measurements show zero resistance (within resolution) and suppression in magnetic fields, thus strongly suggesting superconductivity,” he comments. “It will be exciting to see future work probing other signatures of superconductivity. The X-ray diffraction measurements could be more comprehensive and leave some room for uncertainty to whether it is indeed the claimed LaSc2H24 structure giving rise to the superconductivity.”
Ma and colleagues say they will continue to study the properties of this compound – and in particular, verify the isotope effect (a signature of conventional superconductors) or measure the superconducting critical current. “We will also try to directly detect the Meissner effect – a key goal for high-temperature superhydride superconductors in general,” says Ma. “Guided by rapidly advancing theoretical predictions, we will also synthesize new multinary superhydrides to achieve better superconducting properties under much lower pressures.”
International research collaborations will be increasingly led by scientists in China over the coming decade. That is according to a new study by researchers at the University of Chicago, which finds that the power balance in international science has shifted markedly away from the US and towards China over the last 25 years (Proc. Natl. Acad. Sci. 122 e2414893122).
To explore China’s role in global science, the team used a machine-learning model to predict the lead researchers of almost six million scientific papers that involved international collaboration listed by online bibliographic catalogue OpenAlex. The model was trained on author data from 80 000 papers published in high-profile journals that routinely detail author contributions, including team leadership.
The study found that between 2010 and 2012 there were only 4429 scientists from China who were likely to have led China-US collaborations. By 2023, this number had risen to 12714, meaning that the proportion of team leaders affiliated with Chinese institutions had risen from 30% to 45%.
Key areas
If this trend continues, China will hit “leadership parity” with the US in chemistry, materials science and computer science by 2028, with maths, physics and engineering being level by 2031. The analysis also suggests that China will achieve leadership parity with the US in eight “critical technology” areas by 2030, including AI, semiconductors, communications, energy and high-performance computing.
For China-UK partnerships, the model found that equality had already been reached in 2019, while EU and China leadership roles will be on par this year or next. The authors also found that China has been actively training scientists in nations in the “Belt and Road Initiative” which seeks to connect China closer to the world through investments and infrastructure projects.
This, the researchers warn, limits the ability to isolate science done in China. Instead, they suggest that it could inspire a different course of action, with the US and other countries expanding their engagement with the developing world to train a global workforce and accelerate scientific advancements beneficial to their economies.
This episode explores the scientific and technological significance of 2D materials such as graphene. My guest is Antonio Rossi, who is a researcher in 2D Materials Engineering at the Italian Institute of Technology in Genoa.
Rossi explains why 2D materials are fundamentally different than their 3D counterparts – and how these differences are driving scientific progress and the development of new and exciting technologies.
Graphene is the most famous 2D material and Rossi talks about today’s real-world applications of graphene in coatings. We also chat about the challenges facing scientists and engineers who are trying to exploit graphene’s unique electronic properties.
Rossi’s current research focuses on two other promising 2D materials – tungsten disulfide and hexagonal boron nitride. He explains why tungsten disulphide shows great technological promise because of its favourable electronic and optical properties; and why hexagonal boron nitride is emerging as an ideal substrate for creating 2D devices.
Artificial intelligence (AI) is becoming an important tool in developing new 2D materials. Rossi explains how his team is developing feedback loops that connect AI with the fabrication and characterization of new materials. Our conversation also touches on the use of 2D materials in quantum science and technology.
Microcirculation – the flow of blood through the smallest vessels – is responsible for distributing oxygen and nutrients to tissues and organs throughout the body. Mapping this flow at the whole-organ scale could enhance our understanding of the circulatory system and improve diagnosis of vascular disorders. With this aim, researchers at the Institute Physics for Medicine Paris (Inserm, ESPCI-PSL, CNRS) have combined 3D ultrasound localization microscopy (ULM) with a multi-lens array method to image blood flow dynamics in entire organs with micrometric resolution, reporting their findings in Nature Communications.
“Beyond understanding how an organ functions across different spatial scales, imaging the vasculature of an entire organ reveals the spatial relationships between macro- and micro-vascular networks, providing a comprehensive assessment of its structural and functional organization,” explains senior author Clement Papadacci.
The 3D ULM technique works by localizing intravenously injected microbubbles. Offering a spatial resolution roughly ten times finer than conventional ultrasound, 3D ULM can map and quantify micro-scale vascular structures. But while the method has proved valuable for mapping whole organs in small animals, visualizing entire organs in large animals or humans is hindered by the limitations of existing technology.
To enable wide field-of-view coverage while maintaining high-resolution imaging, the team – led by PhD student Nabil Haidour under Papadacci’s supervision – developed a multi-lens array probe. The probe comprises an array of 252 large (4.5 mm²) ultrasound transducer elements. The use of large elements increases the probe’s sensitive area to a total footprint of 104 x 82 mm, while maintaining a relatively low element count.
Each transducer element is equipped with an individual acoustic diverging lens. “Large elements alone are too directive to create an image, as they cannot generate sufficient overlap or interference between beams,” Papadacci explains. “The acoustic lenses reduce this directivity, allowing the elements to focus and coherently combine signals in reception, thus enabling volumetric image formation.”
Whole-organ imaging
After validating their method via numerical simulations and phantom experiments, the team used a multi-lens array probe driven by a clinical ultrasound system to perform 3D dynamic ULM of an entire explanted porcine heart – considered an ideal cardiac model as its vascular anatomies and dimensions are comparable to those of humans.
The heart was perfused with microbubble solution, enabling the probe to visualize the whole coronary microcirculation network over a large volume of 120 x 100 x 82 mm, with a spatial resolution of around 125 µm. The technique enabled visualization of both large vessels and the finest microcirculation in real time. The team also used a skeletonization algorithm to measure vessel radii at each voxel, which ranged from approximately 75 to 600 µm.
As well as structural imaging, the probe can also assess flow dynamics across all vascular scales, with a high temporal resolution of 312 frames/s. By tracking the microbubbles, the researchers estimated absolute flow velocities ranging from 10 mm/s in small vessels to over 300 mm/s in the largest. They could also differentiate arteries and veins based on the flow direction in the coronary network.
In vivo demonstrations
Next, the researchers used the multi-lens array probe to image the entire kidney and liver of an anaesthetized pig at the Veterinary school of Maison Alfort, with the probe positioned in front of the kidney or liver, respectively, and held using an articulated arm. They employed electrocardiography to synchronize the ultrasound acquisitions with periods of minimal respiratory motion and injected microbubble solution intravenously into the animal’s ear.
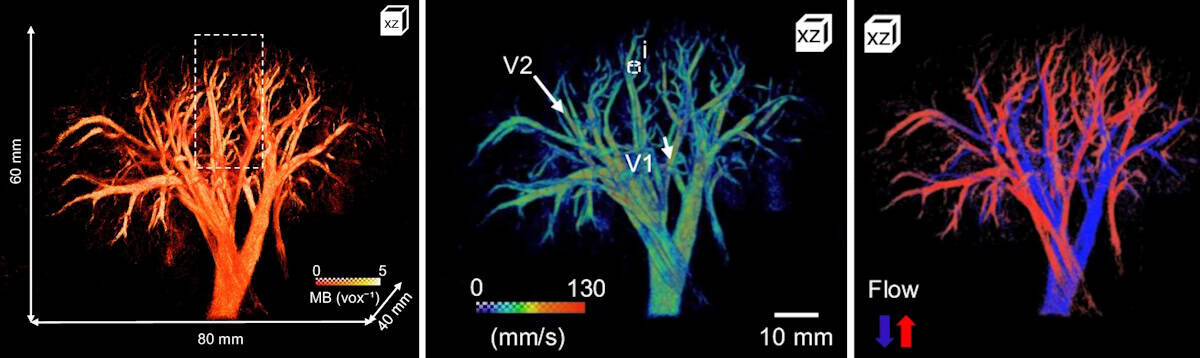
In vivo imaging Left: 3D microbubble density map of the porcine kidney. Centre: 3D flow map of microbubble velocity distribution. Right: 3D flow map showing arterial (red) and venous (blue) flow. (Courtesy: CC BY 4.0/Nat. Commun. 10.1038/s41467-025-64911-z)
The probe mapped the vascular network of the kidney over a 60 x 80 x 40 mm volume with a spatial resolution of 147 µm. The maximum 3D absolute flow velocity was approximately 280 mm/s in the large vessels and the vessel radii ranged from 70 to 400 µm. The team also used directional flow measurements to identify the arterial and venous flow systems.
Liver imaging is more challenging due to respiratory, cardiac and stomach motions. Nevertheless, 3D dynamic ULM enabled high-depth visualization of a large volume of liver vasculature (65 x 100 x 82 mm) with a spatial resolution of 200 µm. Here, the researchers used dynamic velocity measurement to identify the liver’s three blood networks (arterial, venous and portal veins).
“The combination of whole-organ volumetric imaging with high-resolution vascular quantification effectively addresses key limitations of existing modalities, such as ultrasound Doppler imaging, CT angiography and 4D flow MRI,” they write.
Clinical applications of 3D dynamic ULM still need to be demonstrated, but Papadacci suggests that the technique has strong potential for evaluating kidney transplants, coronary microcirculation disorders, stroke, aneurysms and neoangiogenesis in cancer. “It could also become a powerful tool for monitoring treatment response and vascular remodelling over time,” he adds.
Papadacci and colleagues anticipate that translation to human applications will be possible in the near future and plan to begin a clinical trial early in 2026.
Enigmatic Inge Lehmann around the time she quit her job at Denmark’s Geodetic Institute in 1953. (Courtesy: GEUS)
In the 1930s a little-known Danish seismologist calculated that the Earth has a solid inner core, within the liquid outer core identified just a decade earlier. The international scientific community welcomed Inge Lehmann as a member of the relatively new field of geophysics – yet in her home country, Lehmann was never really acknowledged as more than a very competent keeper of instruments.
It was only after retiring from her seismologist job aged 65 that Lehmann was able to devote herself full time to research. For the next 30 years, Lehmann worked and published prolifically, finally receiving awards and plaudits that were well deserved. However, this remarkable scientist, who died in 1993 aged 104, rarely appears in short histories of her field.
In a step to address this, we now have a biography of Lehmann: If I Am Right, and I Know I Am by Hanne Strager, a Danish biologist, science museum director and science writer. Strager pieces together Lehmann’s life in great detail, as well as providing potted histories of the scientific areas that Lehmann contributed to.
A brief glance at the chronology of Lehmann’s education and career would suggest that she was a late starter. She was 32 when she graduated with a bachelor’s degree in mathematics from the University of Copenhagen, 40 when she received her master’s degree in geodosy and was appointed state geodesist for Denmark. Lehmann faced a litany of struggles in her younger years, from health problems and money issues to the restrictions placed on most women’s education in the first decades of the 20th century.
The limits did not come from her family. Lehmann and her sister were sent to good schools, she was encouraged to attend university, and was never pressed to get married, which would likely have meant the end of her education. When she asked her father’s permission to go to the University of Cambridge, his objection was the cost – though the money was found and Lehmann duly went to Newnham College in 1910. While there she passed all the preliminary exams to study for Cambridge’s legendarily tough mathematical tripos but then her health forced her to leave.
Lehmann was suffering from stomach pains; she had trouble sleeping; her hair was falling out. And this was not her first breakdown. She had previously studied for a year at the University of Copenhagen before then, too, dropping out and moving to the countryside to recover her health.
The cause of Lehmann’s recurrent breakdowns is unknown. They unfortunately fed into the prevailing view of the time that women were too fragile for the rigours of higher learning. Strager attempts to unpick these historical attitudes from Lehmann’s very real medical issues. She posits that Lehmann had severe anxiety or a physical limitation to how hard she could push herself. But this conclusion fails to address the hostile conditions Lehmann was working in.
In Cambridge Lehmann formed firm friendships that lasted the rest of her life. But women there did not have the same access to learning as men. They were barred from most libraries and laboratories; could not attend all the lectures; were often mocked and belittled by professors and male students. They could sit exams but, even if they passed, would not be awarded a degree. This was a contributing factor when after the First World War Lehmann decided to complete her undergraduate studies in Copenhagen rather than Cambridge.
More than meets the eye
Lehmann is described as quiet, shy, reticent. But she could be eloquent in writing and once her career began she established connections with scientists all over the world by writing to them frequently. She was also not the wallflower she initially appeared to be. When she was hired as an assistant at Denmark’s Institute for the Measurement of Degrees, she quickly complained that she was being using as an office clerk, not a scientist, and she would not have accepted the job had she known this was the role. She was instead given geometry tasks that she found intellectually stimulating, which led her to seismology.
Unfortunately, soon after this Lehmann’s career development stalled. While her title of “state geodesist” sounds impressive, she was the only seismologist in Denmark for decades, responsible for all the seismographs in Denmark and Greenland. Her days were filled with the practicalities of instrument maintenance and publishing reports of all the data collected.
Intrepid Inge Lehmann at the Ittoqqortootmitt (Scoresbysund) seismic station in Greenland c. 1928. A keen hiker, Lehmann was comfortable in cold and remote environments. (Courtesy: GEUS)
Despite repeated requests Lehmann didn’t receive an assistant, which meant she never got round to completing a PhD, though she did work towards one in her evenings and weekends. Time and again opportunities for career advancement went to men who had the title of doctor but far less real experience in geophysics. Even after she co-founded the Danish Geophysical Society in 1934, her native country overlooked her.
The breakthrough that should have changed this attitude from the men around her came in 1936, when she published “P’ ”. This innocuous sounding paper was revolutionary, but based firmly in the P wave and S wave measurements that Lehmann routinely monitored.
In If I Am Right, and I Know I Am, Strager clearly explains what P and S waves are. She also highlights why they were being studied by both state seismologist Lehmann and Cambridge statistician Harold Jeffreys, and how they led to both scientists’ biggest breakthroughs.
After any seismological disturbance, P and S waves propagate through the Earth. P waves move at different speeds according to the material they encounter, while S waves cannot pass through liquid or air. This knowledge allowed Lehmann to calculate whether any fluctuations in seismograph readings were earthquakes, and if so where the epicentre was located. And it led to Jeffreys’ insight that the Earth must have a liquid core.
Lehmann’s attention to detail meant she spotted a “discontinuity” in P waves that did not quite match a purely liquid core. She immediately wrote to Jeffreys that she believed there was another layer to the Earth, a solid inner core, but he was dismissive – which led to her writing the statement that forms the title of this book. Undeterred, she published her discovery in the journal of the International Union of Geodesy and Geophysics.
Home from home
In 1951 Lehmann visited the institution that would become her second home: the Lamont Geological Observatory in New York state. Its director Maurice Ewing invited her to work there on a sabbatical, arranging all the practicalities of travel and housing on her behalf.
Here, Lehmann finally had something she had lacked her entire career: friendly collaboration with colleagues who not only took her seriously but also revered her. Lehmann took retirement from her job in Denmark and began to spend months of every year at the Lamont Observatory until well into her 80s.
Valued colleague A farewell party held for Inge Lehmann in 1954 at Lamont Geological Observatory after one of her research stays. (Courtesy: GEUS)
Though Strager tells us this “second phase” of Lehmann’s career was prolific, she provides little detail about the work Lehmann did. She initially focused on detecting nuclear tests during the Cold War. But her later work was more varied, and continued after she lost most of her vision. Lehmann published her final paper aged 99.
If I Am Right, and I Know I Am is bookended with accounts of Strager’s research into one particular letter sent to Lehmann, an anonymous (because the final page has been lost) declaration of love. It’s an insight into the lengths Strager went to – reading all the surviving correspondence to and from Lehmann; interviewing living relatives and colleagues; working with historians both professional and amateur; visiting archives in several countries.
But for me it hit the wrong tone. The preface and epilogue are mostly speculation about Lehmann’s love life. Lehmann destroyed a lot of her personal correspondence towards the end of her life, and chose what papers to donate to an archive. To me those are the actions of a woman who wants to control the narrative of her life – and does not want her romances to be written about. I would have preferred instead another chapter about her later work, of which we know she was proud.
But for the majority of its pages, this is a book of which Strager can be proud. I came away from it with great admiration for Lehmann and an appreciation for how lonely life was for many women scientists even in recent history.
The LIGO–Virgo–KAGRA collaboration has detected strong evidence for second-generation black holes, which were formed from earlier mergers of smaller black holes. The two gravitational wave signals provide one of the strongest confirmations to date for how Einstein’s general theory of relativity describes rotating black holes. Studying such objects also provides a testbed for probing new physics beyond the Standard Model.
Over the past decade, the global network of interferometers operated by LIGO, Virgo, and KAGRA have detected close to 300 gravitational waves (GWs) – mostly from the mergers of binary black holes.
In October 2024 the network detected a clear signal that pointed back to a merger that occurred 700 million light-years away. The progenitor black holes were 20 and 6 solar masses and the larger object was spinning at 370 Hz, which makes it one of the fastest-spinning black holes ever observed.
Just one month later, the collaboration detected the coalescence of another highly imbalanced binary (17 and 8 solar masses), 2.4 billion light-years away. This signal was even more unusual – showing for the first time that the larger companion was spinning in the opposite direction of the binary orbit.
Massive and spinning
While conventional wisdom says black holes should not be spinning at such high rates, the observations were not entirely unexpected. “With both events having one black hole, which is both significantly more massive than the other and rapidly spinning, [the observations] provide tantalizing evidence that these black holes were formed from previous black hole mergers,” explains Stephen Fairhurst at Cardiff University, spokesperson of the LIGO Collaboration. If this were the case, the two GW signals – called GW241011 and GW241110 – are first observations of second-generation black holes. This is because when a binary merges, the resulting second-generation object tends to have a large spin.
The GW241011 signal was particularly clear, which allowed the team to make the third-ever observation of higher harmonic modes. These are overtones in the GW signal that become far clearer when the masses of the coalescing bodies are highly imbalanced.
The precision of the GW241011 measurement provides one of the most stringent verifications so far of general relativity. The observations also support Roy Kerr’s prediction that rapid rotation distorts the shape of a black hole.
Kerr and Einstein confirmed
“We now know that black holes are shaped like Einstein and Kerr predicted, and general relativity can add two more checkmarks in its list of many successes,” says team member Carl-Johan Haster at the University of Nevada, Las Vegas. “This discovery also means that we’re more sensitive than ever to any new physics that might lie beyond Einstein’s theory.”
This new physics could include hypothetical particles called ultralight bosons. These could form in clouds just outside the event horizons of spinning black holes, and would gradually drain a black hole’s rotational energy via a quantum effect called superradiance.
The idea is that the observed second-generation black holes had been spinning for billions of years before their mergers occurred. This means that if ultralight bosons were present, they cannot have removed lots of angular momentum from the black holes. This places the tightest constraint to date on the mass of ultralight bosons.
“Planned upgrades to the LIGO, Virgo and KAGRA detectors will enable further observations of similar systems,” Fairhurst says. “They will enable us to better understand both the fundamental physics governing these black hole binaries and the astrophysical mechanisms that lead to their formation.”
Haster adds, “Each new detection provides important insights about the universe, reminding us that each observed merger is both an astrophysical discovery but also an invaluable laboratory for probing the fundamental laws of physics”.
Quantum error correction codes protect quantum information from decoherence and quantum noise, and are therefore crucial to the development of quantum computing and the creation of more reliable and complex quantum algorithms. One example is the five-qubit error correction code, five being the minimum number of qubits required to fix single-qubit errors. These contain five physical qubits (a basic off/on unit of quantum information made using trapped ions, superconducting circuits, or quantum dots) to correct one logical qubit (a collection of physical qubits arranged in such a way as to correct errors). Yet imperfections in the hardware can still lead to quantum errors.
A method of testing quantum error correction codes is self-testing. Self-testing is a powerful tool for verifying quantum properties using only input-output statistics, treating quantum devices as black boxes. It has evolved from bipartite systems consisting of two quantum subsystems, to multipartite entanglement, where entanglement is among three or more subsystems, and now to genuinely entangled subspaces, where every state is fully entangled across all subsystems. Genuinely entangled subspaces offer stronger, guaranteed entanglement than general multipartite states, making them more reliable for quantum computing and error correction.
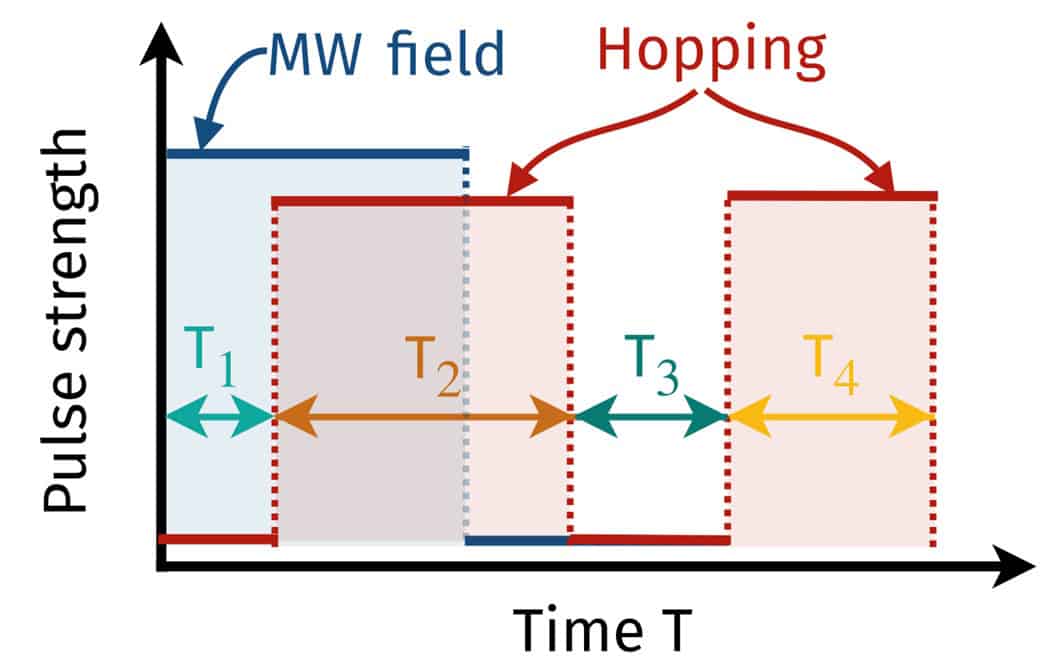
In this research, self-testing techniques are used to certify genuinely entangled logical subspaces within the five-qubit code on photonic and superconducting platforms. This is achieved by preparing informationally complete logical states that span the entire logical space, meaning the set is rich enough to fully characterize the behaviour of the system. They deliberately introduce basic quantum errors by simulating Pauli errors on the physical qubit, which mimics real-world noise. Finally, they use mathematical tests known as Bell inequalities, adapted to the framework used in quantum error correction, to check whether the system evolves in the initial logical subspaces after the errors are introduced.
Extractability measures tell you how close the tested quantum system is to the ideal target state, with 1 being a perfect match. The certification is supported by extractability measures of at least 0.828 ± 0.006 and 0.621 ± 0.007 for the photonic and superconducting systems, respectively. The photonic platform achieved a high extractability score, meaning the logical subspace was very close to the ideal one. The superconducting platform had a lower score but still showed meaningful entanglement. These scores show that the self-testing method works in practice and confirm strong entanglement in the five-qubit code on both platforms.
This research contributes to the advancement of quantum technologies by providing robust methods for verifying and characterizing complex quantum structures, which is essential for the development of reliable and scalable quantum systems. It also demonstrates that device-independent certification can extend beyond quantum states and measurements to more general quantum structures.
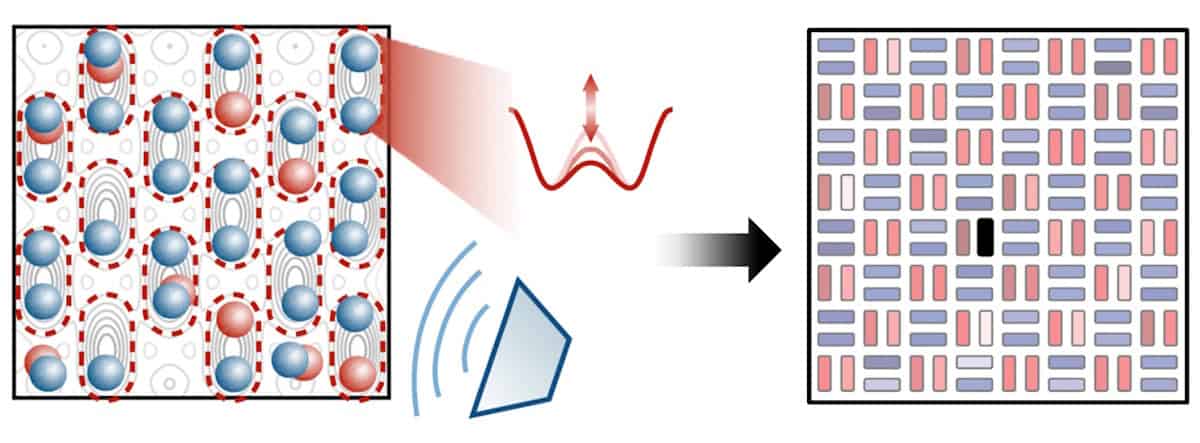
For almost a century, physicists have tried to understand why and how materials become magnetic. From refrigerator magnets to magnetic memories, the microscopic origins of magnetism remain a surprisingly subtle puzzle — especially in materials where electrons behave both like individual particles and like a collective sea.
In most transition-metal compounds, magnetism comes from the dance between localized and mobile electrons. Some electrons stay near their home atoms and form tiny magnetic moments (spins), while others roam freely through the crystal. The interaction between these two types of electrons produces “double-exchange” ferromagnetism — the mechanism that gives rise to the rich magnetic behaviour of materials such as manganites, famous for their colossal magnetoresistance (a dramatic change in electrical resistance under a magnetic field). Traditionally, scientists modelled this behaviour by treating the localized spins as classical arrows — big and well-defined, like compass needles. This approximation works well enough for explaining basic ferromagnetism, but experiments over the last few decades have revealed strange features that defy the classical picture. In particular, neutron scattering studies of manganites showed that the collective spin excitations, called magnons, do not behave as expected. Their energy spectrum “softens” (the waves slow down) and their sharp signals blur into fuzzy continua — a sign that the magnons are losing their coherence. Until now, these effects were usually blamed on vibrations of the atomic lattice (phonons) or on complex interactions between charge, spin, and orbital motion.
Left to right: Adriana Moreo and Elbio Dagotto from University of Tennessee (USA), Takami Tohyama from Tokyo University of Science (Japan), and Marcin Mierzejewski and Jacek Herbrych from Wrocław University of Technology (Courtesy: Herbrych/Wrocław University of Science and Technology)
A new theoretical study challenges that assumption. By going fully quantum mechanical — treating every localized spin not as a classical arrow but as a true quantum object that can fluctuate, entangle, and superpose — the researchers have reproduced these puzzling experimental observations without invoking phonons at all. Using two powerful model systems (a quantum version of the Kondo lattice and a two-orbital Hubbard model), the team simulated how electrons and spins interact when no semiclassical approximations are allowed. The results reveal a subtle quantum landscape. Instead of a single type of electron excitation, the system hosts two. One behaves like a spinless fermion — a charge carrier stripped of its magnetic identity. The other forms a broad, “incoherent” band of excitations arising from local quantum triplets. These incoherent states sit close to the Fermi level and act as a noisy background — a Stoner-like continuum — that the magnons can scatter off. The result: magnons lose their coherence and energy in just the way experiments observe.
Perhaps most surprisingly, this mechanism doesn’t rely on the crystal lattice at all. It’s an intrinsic consequence of the quantum nature of the spins themselves. Larger localized spins, such as those in classical manganites, tend to suppress the effect — explaining why decoherence is weaker in some materials than others. Consequently, the implications reach beyond manganites. Similar quantum interplay may occur in iron-based superconductors, ruthenates, and heavy-fermion systems where magnetism and superconductivity coexist. Even in materials without permanent local moments, strong electronic correlations can generate the same kind of quantum magnetism.
In short, this work uncovers a purely electronic route to complex magnetic dynamics — showing that the quantum personality of the electron alone can mimic effects once thought to require lattice distortions. By uniting electronic structure and spin excitations under a single, fully quantum description, it moves us one step closer to understanding how magnetism truly works in the most intricate materials.
Using a new type of low-power, compact, fluid-based prism to steer the beam in a laser scanning microscope could transform brain imaging and help researchers learn more about neurological conditions such as Alzheimer’s disease.
“We quickly became interested in biological imaging, and work with a neuroscience group at University of Colorado Denver Anschutz Medical Campus that uses mouse models to study neuroscience,” Gopinath tells Physics World. “Neuroscience is not well understood, as illustrated by the neurodegenerative diseases that don’t have good cures. So a great benefit of this technology is the potential to study, detect and treat neurodegenerative diseases such as Alzheimer’s, Parkinson’s and schizophrenia,” she explains.
The researchers fabricated their patented electrowetting prism using custom deposition and lithography methods. The device consists of two immiscible liquids housed in a 5 mm tall, 4 mm diameter glass tube, with a dielectric layer on the inner wall coating four independent electrodes. When an electric field is produced by applying a potential difference between a pair of electrodes on opposite sides of the tube, it changes the surface tension and therefore the curvature of the meniscus between the two liquids. Light passing through the device is refracted by a different amount depending on the angle of tilt of the meniscus (as well as on the optical properties of the liquids chosen), enabling beams to be steered by changing the voltage on the electrodes.
Beam steering for scanning in imaging and microscopy can be achieved via several means, including mechanically controlled mirrors, glass prisms or acousto-optic deflectors (in which a sound wave is used to diffract the light beam). But, unlike the new electrowetting prisms, these methods consume too much power and are not small or lightweight enough to be used for miniature microscopy of neural activity in the brains of living animals.
In tests detailed in Optics Express, the researchers integrated their electrowetting prism into an existing two-photon laser scanning microscope and successfully imaged individual 5 µm-diameter fluorescent polystyrene beads, as well as large clusters of those beads.
They also used computer simulation to study how the liquid–liquid interface moved, and found that when a sinusoidal voltage is used for actuation, at 25 and 75 Hz, standing wave resonance modes occur at the meniscus – a result closely matched by a subsequent experiment that showed resonances at 24 and 72 Hz. These resonance modes are important for enhancing device performance since they increase the angle through which the meniscus can tilt and thus enable optical beams to be steered through a greater range of angles, which helps minimize distortions when raster scanning in two dimensions.
Bright explains that this research built on previous work in which an electrowetting prism was used in a benchtop microscope to image a mouse brain. He cites seeing the individual neurons as a standout moment that, coupled with the current results, shows their prism is now “proven and ready to go”.
Gopinath and Bright caution that “more work is needed to allow human brain scans, such as limiting voltage requirements, allowing the device to operate at safe voltage levels, and miniaturization of the device to allow faster scan speeds and acquiring images at a much faster rate”. But they add that miniaturization would also make the device useful for endoscopy, robotics, chip-scale atomic clocks and space-based communication between satellites.
The team has already begun investigating two other potential applications: LiDAR (light detection and ranging) systems and optical coherence tomography (OCT). Next, the researchers “hope to integrate the device into a miniaturized microscope to allow imaging of the brain in freely moving animals in natural outside environments,” they say. “We also aim to improve the packaging of our devices so they can be integrated into many other imaging systems.”
Marking 100 years since the advent of quantum mechanics, IYQ aims to raise awareness of the impact of quantum physics and its myriad future applications, with a global diary of quantum-themed public talks, scientific conferences, industry events and more.
You can find out more about the contributions of Indian physicist Satyendra Nath Bose to quantum science; explore weird phenomena such as causal order and quantum superposition; and discover the latest applications of quantum computing.
A century after quantum mechanics was first formulated, many physicists are still undecided on some of the most basic foundational questions. There’s no agreement on which interpretation of quantum mechanics holds strong; whether the wavefunction is merely a mathematical tool or a true representation of reality; or what impact an observer has on a quantum state.
Some of the biggest unanswered questions in physics – such as finding the quantum/classical boundary or reconciling gravity and quantum mechanics – lie at the heart of these conundrums. So as we look to the future of quantum – from its fundamentals to its technological applications – let us hope that some answers to these puzzles will become apparent as we crack the quantum code to our universe.
Unless you’ve been living under a stone, you can’t have failed to notice that 2025 marks the first 100 years of quantum mechanics. A massive milestone, to say the least, about which much has been written in Physics World and elsewhere in what is the International Year of Quantum Science and Technology (IYQ). However, I’d like to focus on a specific piece of quantum technology, namely quantum computing.
I keep hearing about quantum computers, so people must be using them to do cool things, and surely they will soon be as commonplace as classical computers. But as a physicist-turned-engineer working in the aerospace sector, I struggle to get a clear picture of where things are really at. If I ask friends and colleagues when they expect to see quantum computers routinely used in everyday life, I get answers ranging from “in the next two years” to “maybe in my lifetime” or even “never”.
Before we go any further, it’s worth reminding ourselves that quantum computing relies on several key quantum properties, including superposition, which gives rise to the quantum bit, or qubit. The basic building block of a quantum computer – the qubit – exists as a combination of 0 and 1 states at the same time and is represented by a probabilistic wave function. Classical computers, in contrast, use binary digital bits that are either 0 or 1.
Also vital for quantum computers is the notion of entanglement, which is when two or more qubits are co-ordinated, allowing them to share their quantum information. In a highly correlated system, a quantum computer can explore many paths simultaneously. This “massive scale” parallel processing is how quantum may solve certain problems exponentially faster than a classical computer.
The other key phenomenon for quantum computers is quantum interference. The wave-like nature of qubits means that when different probability amplitudes are in phase, they combine constructively to increase the likelihood of the right solution. Conversely, destructive interference occurs when amplitudes are out of phase, making it more likely to get the wrong answer.
Quantum interference is important in quantum computing because it allows quantum algorithms to amplify the probability of correct answers and suppress incorrect ones, making calculations much faster. Along with superposition and entanglement, it means that quantum computers could process and store vast numbers of probabilities at once, outstripping even the best classical supercomputers.
Towards real devices
To me, it all sounds exciting, but what have quantum computers ever done for us so far? It’s clear that quantum computers are not ready to be deployed in the real world. Significant technological challenges need to be overcome before they become fully realisable. In any case, no-one is expecting quantum computers to displace classical computers “like for like”: they’ll both be used for different things.
Yet it seems that the very essence of quantum computing is also its Achilles heel. Superposition, entanglement and interference – the quantum properties that will make it so powerful – are also incredibly difficult to create and maintain. Qubits are also extremely sensitive to their surroundings. They easily lose their quantum state due to interactions with the environment, whether via stray particles, electromagnetic fields, or thermal fluctuations. Known as decoherence, it makes quantum computers prone to error.
That’s why quantum computers need specialized – and often cryogenically controlled – environments to maintain the quantum states necessary for accurate computation. Building a quantum system with lots of interconnected qubits is therefore a major, expensive engineering challenge, with complex hardware and extreme operating conditions. Developing “fault-tolerant” quantum hardware and robust error-correction techniques will be essential if we want reliable quantum computation.
As for the development of software and algorithms for quantum systems, there’s a long way to go, with a lack of mature tools and frameworks. Quantum algorithms require fundamentally different programming paradigms to those used for classical computers. Put simply, that’s why building reliable, real-world deployable quantum computers remains a grand challenge.
What does the future hold?
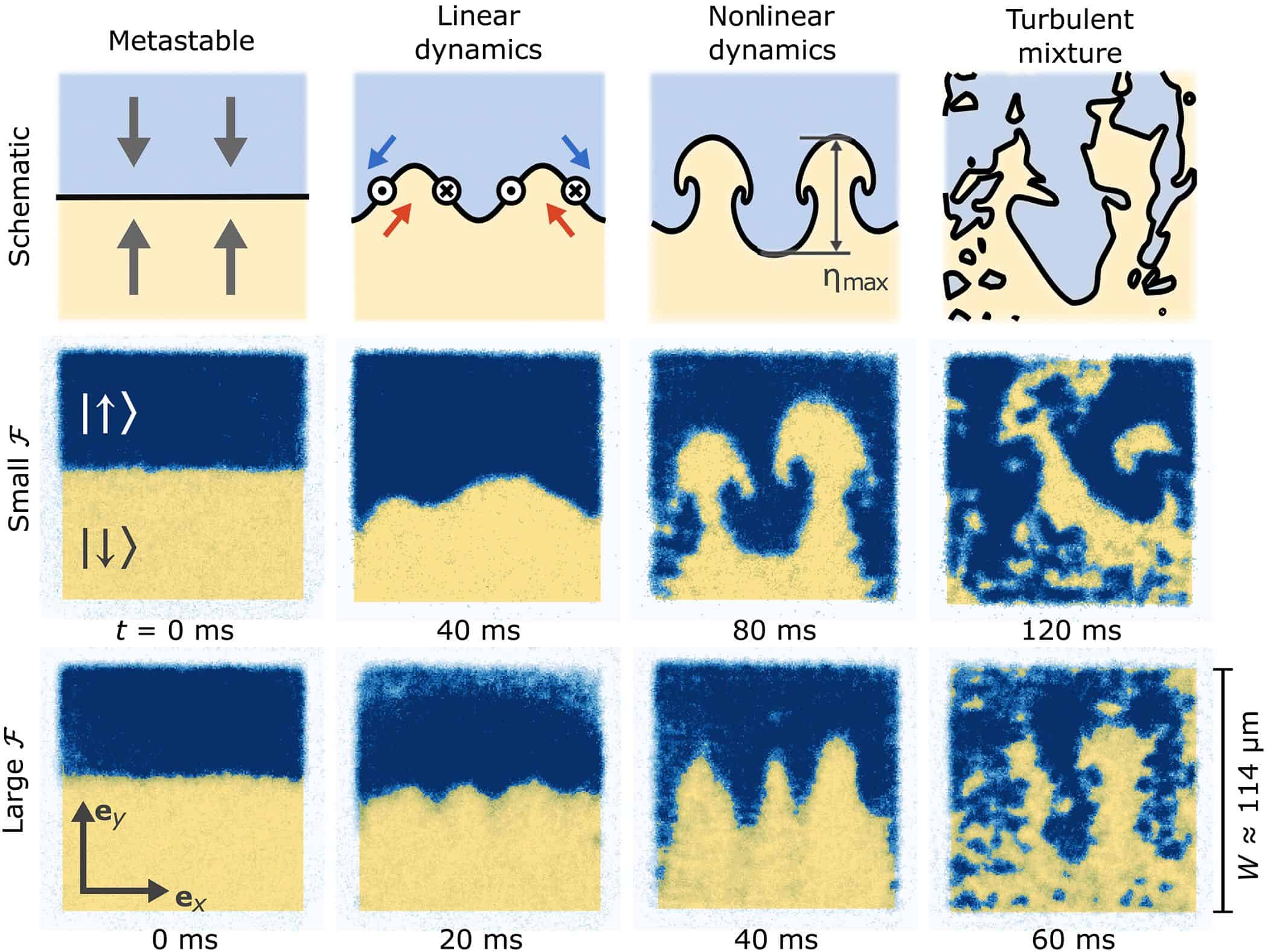
Despite the huge amount of work that still lies in store, quantum computers have already demonstrated some amazing potential. The US firm D-Wave, for example, claimed earlier this year to have carried out simulations of quantum magnetic phase transitions that wouldn’t be possible with the most powerful classical devices. If true, this was the first time a quantum computer had achieved “quantum advantage” for a practical physics problem (whether the problem was worth solving is another question).
There is also a lot of research and development going on around the world into solving the qubit stability problem. At some stage, there will likely be a breakthrough design for robust and reliable quantum computer architecture. There is probably a lot of technical advancement happening right now behind closed doors.
The first real-world applications of quantum computers will be akin to the giant classical supercomputers of the past. If you were around in the 1980s, you’ll remember Cray supercomputers: huge, inaccessible beasts owned by large corporations, government agencies and academic institutions to enable vast amounts of calculations to be performed (provided you had the money).
And, if I believe what I read, quantum computers will not replace classical computers, at least not initially, but work alongside them, as each has its own relative strengths. Quantum computers will be suited for specific and highly demanding computational tasks, such as drug discovery, materials science, financial modelling, complex optimization problems and increasingly large artificial intelligence and machine-learning models.
These are all things beyond the limits of classical computer resource. Classical computers will remain relevant for everyday tasks like web browsing, word processing and managing databases, and they will be essential for handling the data preparation, visualization and error correction required by quantum systems.
And there is one final point to mention, which is cyber security. Quantum computing poses a major threat to existing encryption methods, with potential to undermine widely used public-key cryptography. There are concerns that hackers nowadays are storing their stolen data in anticipation of future quantum decryption.
Having looked into the topic, I can now see why the timeline for quantum computing is so fuzzy and why I got so many different answers when I asked people when the technology would be mainstream. Quite simply, I still can’t predict how or when the tech stack will pan out. But as IYQ draws to a close, the future for quantum computers is bright.
Modular and scalable: the ICE-Q cryogenics platform delivers the performance and reliability needed for professional computing environments while also providing a flexible and extendable design. The standard configuration includes a cooling module, a payload with a large sample space, and a side-loading wiring module for scalable connectivity (Courtesy: ICEoxford)
At the centre of most quantum labs is a large cylindrical cryostat that keeps the delicate quantum hardware at ultralow temperatures. These cryogenic chambers have expanded to accommodate larger and more complex quantum systems, but the scientists and engineers at UK-based cryogenics specialist ICEoxford have taken a radical new approach to the challenge of scalability. They have split the traditional cryostat into a series of cube-shaped modules that slot into a standard 19-inch rack mount, creating an adaptable platform that can easily be deployed alongside conventional computing infrastructure.
“We wanted to create a robust, modular and scalable solution that enables different quantum technologies to be integrated into the cryostat,” says Greg Graf, the company’s engineering manager. “This approach offers much more flexibility, because it allows different modules to be used for different applications, while the system also delivers the efficiency and reliability that are needed for operational use.”
The standard configuration of the ICE-Q platform has three separate modules: a cryogenics unit that provides the cooling power, a large payload for housing the quantum chip or experiment, and a patent-pending wiring module that attaches to the side of the payload to provide the connections to the outside world. Up to four of these side-loading wiring modules can be bolted onto the payload at the same time, providing thousands of external connections while still fitting into a standard rack. For applications where space is not such an issue, the payload can be further extended to accommodate larger quantum assemblies and potentially tens of thousands of radio-frequency or fibre-optic connections.
The cube-shaped form factor provides much improved access to these external connections, whether for designing and configuring the system or for ongoing maintenance work. The outer shell of each module consists of panels that are easily removed, offering a simple mechanism for bolting modules together or stacking them on top of each other to provide a fully scalable solution that grows with the qubit count.
The flexible design also offers a more practical solution for servicing or upgrading an installed system, since individual modules can be simply swapped over as and when needed. “For quantum computers running in an operational environment it is really important to minimize the downtime,” says Emma Yeatman, senior design engineer at ICEoxford. “With this design we can easily remove one of the modules for servicing, and replace it with another one to keep the system running for longer. For critical infrastructure devices, it is possible to have built-in redundancy that ensures uninterrupted operation in the event of a failure.”
Other features have been integrated into the platform to make it simple to operate, including a new software system for controlling and monitoring the ultracold environment. “Most of our cryostats have been designed for researchers who really want to get involved and adapt the system to meet their needs,” adds Yeatman. “This platform offers more options for people who want an out-of-the-box solution and who don’t want to get hands on with the cryogenics.”
Such a bold design choice was enabled in part by a collaborative research project with Canadian company Photonic Inc, funded jointly by the UK and Canada, that was focused on developing an efficient and reliable cryogenics platform for practical quantum computing. That R&D funding helped to reduce the risk of developing an entirely new technology platform that addresses many of the challenges that ICEoxford and its customers had experienced with traditional cryostats. “Quantum technologies typically need a lot of wiring, and access had become a real issue,” says Yeatman. “We knew there was an opportunity to do better.”
However, converting a large cylindrical cryostat into a slimline and modular form factor demanded some clever engineering solutions. Perhaps the most obvious was creating a frame that allows the modules to be bolted together while still remaining leak tight. Traditional cryostats are welded together to ensure a leak-proof seal, but for greater flexibility the ICEoxford team developed an assembly technique based on mechanical bonding.
The side-loading wiring module also presented a design challenge. To squeeze more wires into the available space, the team developed a high-density connector for the coaxial cables to plug into. An additional cold-head was also integrated into the module to pre-cool the cables, reducing the overall heat load generated by such large numbers of connections entering the ultracold environment.
Flexible for the future: the outer shell of the modules is covered with removable panels that make it easy to extend or reconfigure the system (Courtesy: ICEoxford)
Meanwhile, the speed of the cooldown and the efficiency of operation have been optimized by designing a new type of heat exchanger that is fabricated using a 3D printing process. “When warm gas is returned into the system, a certain amount of cooling power is needed just to compress and liquefy that gas,” explains Kelly. “We designed the heat exchangers to exploit the returning cold gas much more efficiently, which enables us to pre-cool the warm gas and use less energy for the liquefaction.”
The initial prototype has been designed to operate at 1 K, which is ideal for the photonics-based quantum systems being developed by ICEoxford’s research partner. But the modular nature of the platform allows it to be adapted to diverse applications, with a second project now underway with the Rutherford Appleton Lab to develop a module that that will be used at the forefront of the global hunt for dark matter.
Already on the development roadmap are modules that can sustain temperatures as low as 10 mK – which is typically needed for superconducting quantum computing – and a 4 K option for trapped-ion systems. “We already have products for each of those applications, but our aim was to create a modular platform that can be extended and developed to address the changing needs of quantum developers,” says Kelly.
As these different options come onstream, the ICEoxford team believes that it will become easier and quicker to deliver high-performance cryogenic systems that are tailored to the needs of each customer. “It normally takes between six and twelve months to build a complex cryogenics system,” says Graf. “With this modular design we will be able to keep some of the components on the shelf, which would allow us to reduce the lead time by several months.”
More generally, the modular and scalable platform could be a game-changer for commercial organizations that want to exploit quantum computing in their day-to-day operations, as well as for researchers who are pushing the boundaries of cryogenics design with increasingly demanding specifications. “This system introduces new avenues for hardware development that were previously constrained by the existing cryogenics infrastructure,” says Kelly. “The ICE-Q platform directly addresses the need for colder base temperatures, larger sample spaces, higher cooling powers, and increased connectivity, and ensures our clients can continue their aggressive scaling efforts without being bottlenecked by their cooling environment.”
You can find out more about the ICE-Q platform by contacting the ICEoxford team at iceoxford.com, or via email at sales@iceoxford.com. They will also be presenting the platform at the UK’s National Quantum Technologies Showcase in London on 7 November, with a further launch at the American Physical Society meeting in March 2026.
Due to government shutdown restrictions currently in place in the US, the researchers who headed up this study have not been able to comment on their work
Laser plasma acceleration (LPA) may be used to generate multi-gigaelectronvolt muon beams, according to physicists at the Lawrence Berkeley National Laboratory (LBNL) in the US. Their work might help in the development of ultracompact muon sources for applications such as muon tomography – which images the interior of large objects that are inaccessible to X-ray radiography.
Muons are charged subatomic particles that are produced in large quantities when cosmic rays collide with atoms 15–20 km high up in the atmosphere. Muons have the same properties as electrons but are around 200 times heavier. This means they can travel much further through solid structures than electrons. This property is exploited in muon tomography, which analyses how muons penetrate objects and then exploits this information to produce 3D images.
The technique is similar to X-ray tomography used in medical imaging, with the cosmic-ray radiation taking the place of artificially generated X-rays and muon trackers the place of X-ray detectors. Indeed, depending on their energy, muons can traverse metres of rock or other materials, making them ideal for imaging thick and large structures. As a result, the technique has been used to peer inside nuclear reactors, pyramids and volcanoes.
As many as 10,000 muons from cosmic rays reach each square metre of the Earth’s surface every minute. These naturally produced particles have unpredictable properties, however, and they also only come from the vertical direction. This fixed directionality means that can take months to accumulate enough data for tomography.
Another option is to use the large numbers of low-energy muons that can be produced in proton accelerator facilities by smashing a proton beam onto a fixed carbon target. However, these accelerators are large and expensive facilities, limiting their use in muon tomography.
A new compact source
Physicists led by Davide Terzani have now developed a new compact muon source based on LPA-generated electron beams. Such a source, if optimized, could be deployed in the field and could even produce muon beams in specific directions.
In LPA, an ultra-intense, ultra-short, and tightly focused laser pulse propagates into an “under-dense” gas. The pulse’s extremely high electric field ionizes the gas atoms, freeing the electrons from the nuclei, so generating a plasma. The ponderomotive force, or radiation pressure, of the intense laser pulse displaces these electrons and creates an electrostatic wave that produces accelerating fields orders of magnitude higher than what is possible in the traditional radio-frequency cavities used in conventional accelerators.
LPAs have all the advantages of an ultra-compact electron accelerator that allows for muon production in a small-size facility such as BeLLA, where Terzani and his colleagues work. Indeed, in their experiment, they succeeded in generating a 10 GeV electron beam in a 30 cm gas target for the first time.
The researchers collided this beam with a dense target, such as tungsten. This slows the beam down so that it emits Bremsstrahlung, or braking radiation, which interacts with the material, producing secondary products that include lepton–antilepton pairs, such as electron–positron and muon–antimuon pairs. Behind the converter target, there is also a short-lived burst of muons that propagates roughly along the same axis as the incoming electron beam. A thick concrete shielding then filters most of the secondary products, letting the majority of muons pass through it.
Crucially, Terzani and colleagues were able to separate the muon signal from the large background radiation – something that can be difficult to do because of the inherent inefficiency of the muon production process. This allowed them to identify two different muon populations coming from the accelerator. These were a collimated, forward directed population, generated by pair production; and a low-energy, isotropic, population generated by meson decay.
Many applications
Muons can ne used in a range of fields, from imaging to fundamental particle physics. As mentioned, muons from cosmic rays are currently used to inspect large and thick objects not accessible to regular X-ray radiography – a recent example of this is the discovery of a hidden chamber in Khufu’s Pyramid. They can also be used to image the core of a burning blast furnace or nuclear waste storage facilities.
While the new LPA-based technique cannot yet produce muon fluxes suitable for particle physics experiments – to replace a muon injector, for example – it could offer the accelerator community a convenient way to test and develop essential elements towards making a future muon collider.
The experiment in this study, which is detailed in Physical Review Accelerators and Beams, focused on detecting the passage of muons, unequivocally proving their signature. The researchers conclude that they now have a much better understanding of the source of these muons.
Unfortunately, the original programme that funded this research has ended, so future studies are limited at the moment. Not to be disheartened, the researchers say they strongly believe in the potential of LPA-generated muons and are working on resuming some of their experiments. For example, they aim to measure the flux and the spectrum of the resulting muon beam using completely different detection techniques based on ultra-fast particle trackers, for example.
The LBNL team also wants to explore different applications, such as imaging deep ore deposits – something that will be quite challenging because it poses strict limitations on the minimum muon energy required to penetrate soil. Therefore, they are looking into how to increase the muon energy of their source.
When it comes to building a fully functional “fault-tolerant” quantum computer, companies and government labs all over the world are rushing to be the first over the finish line. But a truly useful universal quantum computer capable of running complex algorithms would have to entangle millions of coherent qubits, which are extremely fragile. Because of environmental factors such as temperature, interference from other electronic systems in hardware, and even errors in measurement, today’s devices would fail under an avalanche of errors long before reaching that point.
So the problem of error correction is a key issue for the future of the market. It arises because errors in qubits can’t be corrected simply by keeping multiple copies, as they are in classical computers: quantum rules forbid the copying of qubit states while they are still entangled with others, and are thus unknown. To run quantum circuits with millions of gates, we therefore need new tricks to enable quantum error correction (QEC).
Protected states
The general principle of QEC is to spread the information over many qubits so that an error in any one of them doesn’t matter too much. “The essential idea of quantum error correction is that if we want to protect a quantum system from damage then we should encode it in a very highly entangled state,” says John Preskill, director of the Institute for Quantum Information and Matter at the California Institute of Technology in Pasadena.
There is no unique way of achieving that spreading, however. Different error-correcting codes can depend on the connectivity between qubits – whether, say, they are coupled only to their nearest neighbours or to all the others in the device – which tends to be determined by the physical platform being used. However error correction is done, it must be done fast. “The mechanisms for error correction need to be running at a speed that is commensurate with that of the gate operations,” saysMichael Cuthbert, founding director of the UK’s National Quantum Computing Centre (NQCC). “There’s no point in doing a gate operation in a nanosecond if it then takes 100 microseconds to do the error correction for the next gate operation.”
At the moment, dealing with errors is largely about compensation rather than correction: patching up the problems of errors in retrospect, for example by using algorithms that can throw out some results that are likely to be unreliable (an approach called “post-selection”). It’s also a matter of making better qubits that are less error-prone in the first place.
Qubits are so fragile that their quantum state is very susceptible to the local environment, and can easily be lost through the process of decoherence. Current quantum computers therefore have very high error rates – roughly one error in every few hundred operations. For quantum computers to be truly useful, this error rate will have to be reduced to the scale of one in a million; especially as larger more complex algorithms would require one in a billion or even trillion error rates. This requires real-time quantum error correction (QEC).
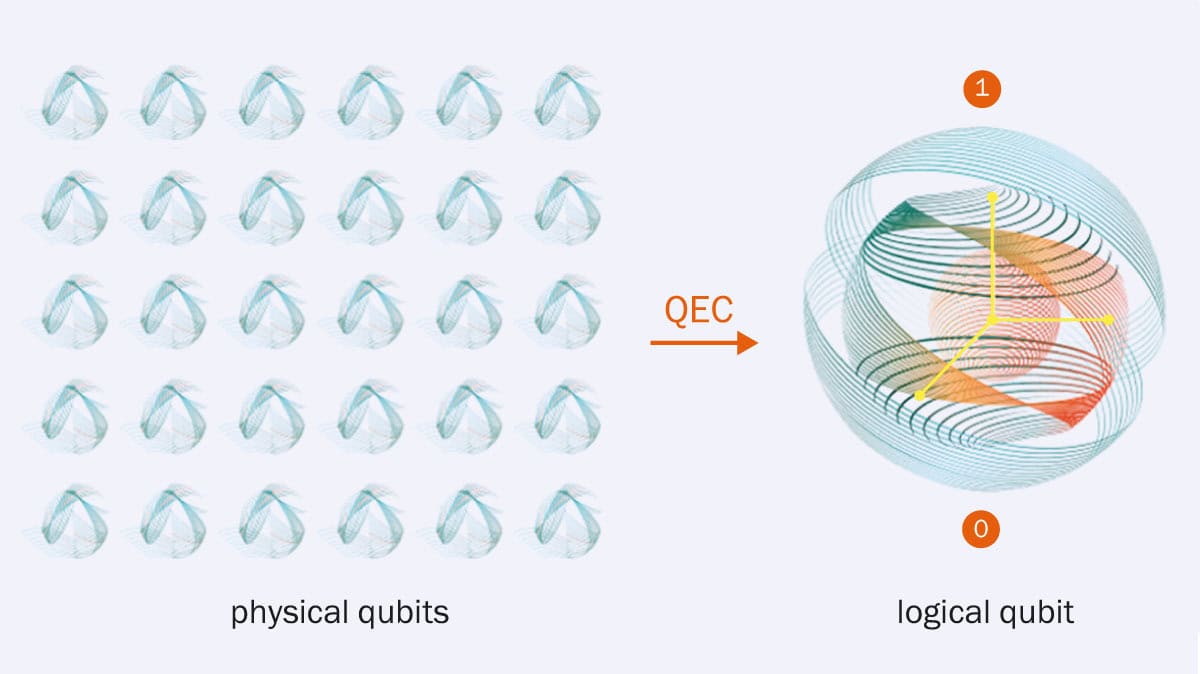
To protect the information stored in qubits, a multitude of unreliable physical qubits have to be combined in such a way that if one qubit fails and causes an error, the others can help protect the system. Essentially, by combining many physical qubits (shown above on the left), one can build a few “logical” qubits that are strongly resistant to noise.
According to Maria Maragkou, commercial vice-president of quantum error-correction company Riverlane, the goal of full QEC has ramifications for the design of the machines all the way from hardware to workflow planning. “The shift to support error correction has a profound effect on the way quantum processors themselves are built, the way we control and operate them, through a robust software stack on top of which the applications can be run,” she explains. The “stack” includes everything from programming languages to user interfaces and servers.
With genuinely fault-tolerant qubits, errors can be kept under control and prevented from proliferating during a computation. Such qubits might be made in principle by combining many physical qubits into a single “logical qubit” in which errors can be corrected (see figure 1). In practice, though, this creates a large overhead: huge numbers of physical qubits might be needed to make just a few fault-tolerant logical qubits. The question is then whether errors in all those physical qubits can be checked faster than they accumulate (see figure 2).
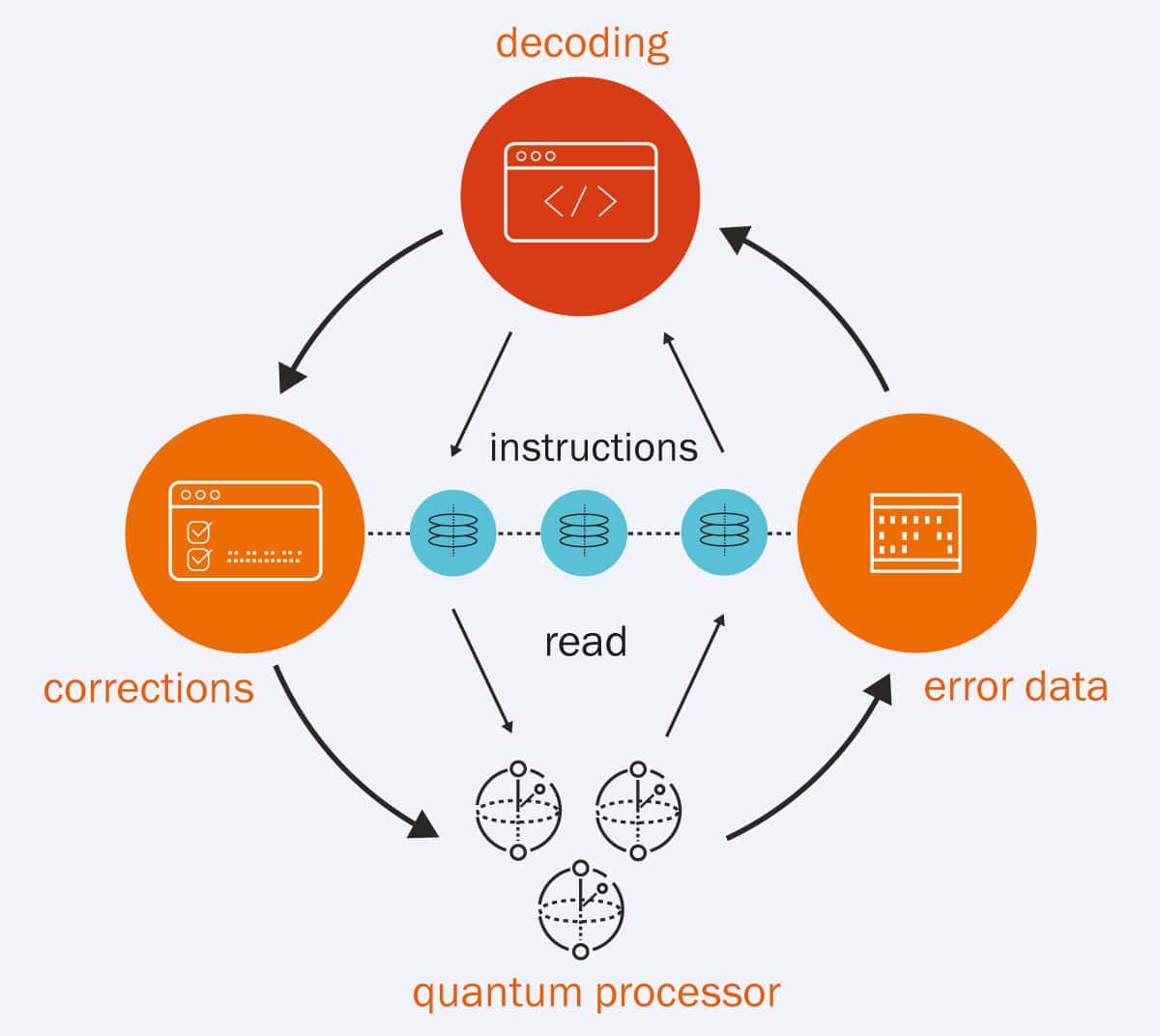
The illustration gives an overview of quantum error correction (QEC) in action within a quantum processing unit. UK-based company Riverlane is building its Deltaflow QEC stack that will correct millions of data errors in real time, allowing a quantum computer to go beyond the reach of any classical supercomputer.
Fault-tolerant quantum computing is the ultimate goal, says Jay Gambetta, director of IBM research at the company’s centre in Yorktown Heights, New York. He believes that to perform truly transformative quantum calculations, the system must go beyond demonstrating a few logical qubits – instead, you need arrays of at least a 100 of them, that can perform more than 100 million quantum operations (108 QuOps). “The number of operations is the most important thing,” he says.
It sounds like a tall order, but Gambetta is confident that IBM will achieve these figures by 2029. By building on what has been achieved so far with error correction and mitigation, he feels “more confident than I ever did before that we can achieve a fault-tolerant computer.” Jerry Chow, previous manager of the Experimental Quantum Computing group at IBM, shares that optimism. “We have a real blueprint for how we can build [such a machine] by 2029,” he says (see figure 3).
Others suspect the breakthrough threshold may be a little lower: Steve Brierley, chief executive of Riverlane, believes that the first error-corrected quantum computer, with around 10 000 physical qubits supporting 100 logical qubits and capable of a million QuOps (a megaQuOp), could come as soon as 2027. Following on, gigaQuOp machines (109 QuOps) should be available by 2030–32, and teraQuOps (1012 QuOp) by 2035–37.
Platform independent
Error mitigation and error correction are just two of the challenges for developers of quantum software. Fundamentally, to develop a truly quantum algorithm involves taking full advantage of the key quantum-mechanical properties such as superposition and entanglement. Often, the best way to do that depends on the hardware used to run the algorithm. But ultimately the goal will be to make software that is not platform-dependent and so doesn’t require the user to think about the physics involved.
“At the moment, a lot of the platforms require you to come right down into the quantum physics, which is a necessity to maximize performance,” says Richard Murray of photonic quantum-computing company Orca. Try to generalize an algorithm by abstracting away from the physics and you’ll usually lower the efficiency with which it runs. “But no user wants to talk about quantum physics when they’re trying to do machine learning or something,” Murray adds. He believes that ultimately it will be possible for quantum software developers to hide those details from users – but Brierly thinks this will require fault-tolerant machines.
“In due time everything below the logical circuit will be a black box to the app developers”, adds Maragkou over at Riverlane. “They will not need to know what kind of error correction is used, what type of qubits are used, and so on.” She stresses that creating truly efficient and useful machines depends on developing the requisite skills. “We need to scale up the workforce to develop better qubits, better error-correction codes and decoders, write the software that can elevate those machines and solve meaningful problems in a way that they can be adopted.” Such skills won’t come only from quantum physicists, she adds: “I would dare say it’s mostly not!”
Yet even now, working on quantum software doesn’t demand a deep expertise in quantum theory. “You can be someone working in quantum computing and solving problems without having a traditional physics training and knowing about the energy levels of the hydrogen atom and so on,” says Ashley Montanaro, who co-founded the quantum software company Phasecraft.
On the other hand, insights can flow in the other direction too: working on quantum algorithms can lead to new physics. “Quantum computing and quantum information are really pushing the boundaries of what we think of as quantum mechanics today,” says Montanaro, adding that QEC “has produced amazing physics breakthroughs.”
Early adopters?
Once we have true error correction, Cuthbert at the UK’s NQCC expects to see “a flow of high-value commercial uses” for quantum computers. What might those be?
In this arena of quantum chemistry and materials science, genuine quantum advantage – calculating something that is impossible using classical methods alone – is more or less here already, says Chow. Crucially, however, quantum methods needn’t be used for the entire simulation but can be added to classical ones to give them a boost for particular parts of the problem.
Joint effort In June 2025, IBM in the US and Japan’s national research laboratory RIKEN, unveiled the IBM Quantum System Two, the first to be used outside the US. It involved IBM’s 156-qubit IBM Heron quantum computing system (left) being paired with RIKEN’s supercomputer Fugaku (right) — one of the most powerful classical systems on Earth. The computers are linked through a high-speed network at the fundamental instruction level to form a proving ground for quantum-centric supercomputing. (Courtesy: IBM and RIKEN)
For example, last year researchers at IBM teamed up with scientists at several RIKEN institutes in Japan to calculate the minimum energy state for the iron sulphide cluster (4Fe-4S) at the heart of the bacterial nitrogenase enzyme that fixes nitrogen. This cluster is too big and complex to be accurately simulated using the classical approximations of quantum chemistry. The researchers used a combination of both quantum computing (with IBM’s 72-qubit Heron chip) and RIKEN’s Fugaku high performance computing (HPC). This idea of “improving classical methods by injecting quantum as a subroutine” is likely to be a more general strategy, says Gambetta. “The future of computing is going to be heterogeneous accelerators [of discovery] that include quantum.”
Likewise, Montanaro says that Phasecraft is developing “quantum-enhanced algorithms”, where a quantum computer is used, not to solve the whole problem, but just to help a classical computer in some way. “There are only certain problems where we know quantum computing is going to be useful,” he says. “I think we are going to see quantum computers working in tandem with classical computers in a hybrid approach. I don’t think we’ll ever see workloads that are entirely run using a quantum computer.” Among the first important problems that quantum machines will solve, according to Montanaro, are the simulation of new materials – to develop, for example, clean-energy technologies (see figure 4).
“For a physicist like me,” says Preskill, “what is really exciting about quantum computing is that we have good reason to believe that a quantum computer would be able to efficiently simulate any process that occurs in nature.”
3 Structural insights
(Courtesy: Phasecraft)
A promising application of quantum computers is simulating novel materials. Researchers from the quantum algorithms firm Phasecraft, for example, have already shown how a quantum computer could help simulate complex materials such as the polycrystalline compound LK-99, which was purported by some researchers in 2024 to be a room-temperature superconductor.
Using a classical/quantum hybrid workflow, together with the firm’s proprietary material simulation approach to encode and compile materials on quantum hardware, Phasecraft researchers were able to establish a classical model of the LK99 structure that allowed them to extract an approximate representation of the electrons within the material. The illustration above shows the green and blue electronic structure around red and grey atoms in LK-99.
Montanaro believes another likely near-term goal for useful quantum computing is solving optimization problems – both here and in quantum simulation, “we think genuine value can be delivered already in this NISQ era with hundreds of qubits.” (NISQ, a term coined by Preskill, refers to noisy intermediate-scale quantum computing, with relatively small numbers of rather noisy, error-prone qubits.)
One further potential benefit of quantum computing is that it tends to require less energy than classical high-performance computing, which is notoriously high. If the energy cost could be cut by even a few percent, it would be worth using quantum resources for that reason alone. “Quantum has real potential for an energy advantage,” says Chow. One study in 2020 showed that a particular quantum-mechanical calculation carried out on a HPC used many orders of magnitude more energy than when it was simulated on a quantum circuit. Such comparisons are not easy, however, in the absence of an agreed and well-defined metric for energy consumption.
Building the market
Right now, the quantum computing market is in a curious superposition of states itself – it has ample proof of principle, but today’s devices are still some way from being able to perform a computation relevant to a practical problem that could not be done with classical computers. Yet to get to that point, the field needs plenty of investment.
The fact that quantum computers, especially if used with HPC, are already unique scientific tools should establish their value in the immediate term, says Gambetta. “I think this is going to accelerate, and will keep the funding going.” It is why IBM is focusing on utility-scale systems of around 100 qubits or so and more than a thousand gate operations, he says, rather than simply trying to build ever bigger devices.
Montanaro sees a role for governments to boost the growth of the industry “where it’s not the right fit for the private sector”. One role of government is simply as a customer. For example, Phasecraft is working with the UK national grid to develop a quantum algorithm for optimizing the energy network. “Longer-term support for academic research is absolutely critical,” Montanaro adds. “It would be a mistake to think that everything is done in terms of the underpinning science, and governments should continue to support blue-skies research.”
The road ahead IBM’s current roadmap charts how the company plans on scaling up its devices to achieve a fault-tolerant device by 2029. Alongside hardware development, the firm will also focus on developing new algorithms and software for these devices. (Courtesy: IBM)
It’s not clear, though, whether there will be a big demand for quantum machines that every user will own and run. Before 2010, “there was an expectation that banks and government departments would all want their own machine – the market would look a bit like HPC,” Cuthbert says. But that demand depends in part on what commercial machines end up being like. “If it’s going to need a premises the size of a football field, with a power station next to it, that becomes the kind of infrastructure that you only want to build nationally.” Even for smaller machines, users are likely to try them first on the cloud before committing to installing one in-house.
According to Cuthbert , the real challenge in the supply-chain development is that many of today’s technologies were developed for the science community – where, say, achieving millikelvin cooling or using high-power lasers is routine. “How do you go from a specialist scientific clientele to something that starts to look like a washing machine factory, where you can make them to a certain level of performance,” while also being much cheaper, and easier to use?
But Cuthbert is optimistic about bridging this gap to get to commercially useful machines, encouraged in part by looking back at the classical computing industry of the 1970s. “The architects of those systems could not imagine what we would use our computation resources for today. So I don’t think we should be too discouraged that you can grow an industry when we don’t know what it’ll do in five years’ time.”
Montanaro too sees analogies with those early days of classical computing. “If you think what the computer industry looked like in the 1940s, it’s very different from even 20 years later. But there are some parallels. There are companies that are filling each of the different niches we saw previously, there are some that are specializing in quantum hardware development, there are some that are just doing software.” Cuthbert thinks that the quantum industry is likely to follow a similar pathway, “but more quickly and leading to greater market consolidation more rapidly.”
However, while the classical computing industry was revolutionized by the advent of personal computing in the 1970s and 80s, it seems very unlikely that we will have any need for quantum laptops. Rather, we might increasingly see apps and services appear that use cloud-based quantum resources for particular operations, merging so seamlessly with classical computing that we don’t even notice.
That, perhaps, would be the ultimate sign of success: that quantum computing becomes invisible, no big deal but just a part of how our answers are delivered.
In the first instalment of this two-part article, Philip Ball explores the latest developments in the quantum-computing industry
When a star rapidly accumulates gas and dust during its early growth phase, it’s called an accretion burst. Now, for the first time, astronomers have observed a planet doing the same thing. The discovery, made using the European Southern Observatory’s Very Large Telescope (VLT) and the James Webb Space Telescope (JWST), shows that the infancy of certain planetary-mass objects and that of newborn stars may share similar characteristics.
Like other rogue planets, Cha1107-7626 was known to be surrounded by a disk of dust and gas. When material from this disk spirals, or accretes, onto the planet, the planet grows.
What Almendros-Abad and colleagues discovered is that this process is not uniform. Using the VLT’s XSHOOTER and the NIRSpec and MIRI instruments on JWST, they found that Cha1107-7626 experienced a burst of accretion beginning in June 2025. This is the first time anyone has seen an accretion burst in an object with such a low mass, and the peak accretion rate of six billion tonnes per second makes it the strongest accretion episode ever recorded in a planetary-mass object. It may not be over, either. At the end of August, when the observing campaign ended, the burst was still ongoing.
An infancy similar to a star’s
The team identified several parallels between Cha1107-7626’s accretion burst and those that young stars experience. Among them were clear signs that gas is being funnelled onto the planet. “This indicates that magnetic fields structure the flow of gas, which is again something well known from stars,” explains Scholz. “Overall, our discovery is establishing interesting, perhaps surprising parallels between stars and planets, which I’m not sure we fully understand yet.”
The astronomers also found that the chemistry of the disc around the planet changed during accretion, with water being present in this phase even though it hadn’t been before. This effect has previously been spotted in stars, but never in a planet until now.
“We’re struck by quite how much the infancy of free-floating planetary-mass objects resembles that of stars like the Sun,” Jayawardhana says. “Our new findings underscore that similarity and imply that some objects comparable to giant planets form the way stars do, from contracting clouds of gas and dust accompanied by disks of their own, and they go through growth episodes just like newborn stars.”
The researchers have been studying similar objects for many years and earlier this year published results based on JWST observations that featured a small sample of planetary-mass objects. “This particular study is part of that sample,” Scholz tells Physics World, “and we obtained the present results because Victor wanted to look in detail at the accretion flow onto Cha1107-7626, and in the process discovered the burst.”
The researchers say they are “keeping an eye” on Cha1107-7626 and other such objects that are still growing because their environment is dynamic and unstable. “More to the point, we really don’t understand what drives these accretion events, and we need detailed follow-up to figure out the underlying reasons for these processes,” Scholz says.
It’s Halloween today and so what better time than to bring you a couple of spooky stories from the world of physics.
First up is researchers at the University of Georgia in the US who have confirmed that six different species of bats found in North America emit a ghoulish green light when exposed to ultraviolet light.
The researchers examined 60 specimens from the Georgia Museum of Natural History and exposed the bats to UV light.
They found that the wings and hind limbs of six species – big brown bats, eastern red bats, Seminole bats, southeastern myotis, grey bats and the Brazilian free-tailed bat – gave off photoluminescence with the resulting glow being a shade of green.
While previous research found that some mammals, like pocket gophers, also emit a glow under ultraviolet light, this was the first discovery of such a phenomenon for bats located in North America.
The colour and location of the glow on the winged mammals suggest it is not down to genetics or camouflage and as it is the same between sexes it is probably not used to attract mates.
Given that many bats can see the wavelengths emitted, one option is that the glow may be an inherited trait used for communication.
“The data suggests that all these species of bats got it from a common ancestor. They didn’t come about this independently,” adds Castleberry. “It may be an artifact now, since maybe glowing served a function somewhere in the evolutionary past, and it doesn’t anymore.”
Thread lightly
In other frightful news, spider webs are a classic Halloween decoration and while the real things are marvels of bioengineering, there is still more to understand about these sticky structures.
Many spider species build spiral wheel-shaped webs – orb webs – to capture prey, and some incorporate so-called “stabilimenta” into their web structure. These “extra touches” look like zig-zagging threads that span the gap between two adjacent “spokes,” or threads arranged in a circular “platform” around the web center.
The purpose of stabilimenta is unknown and proposed functions include as a deterrence for predatory wasps or birds.
Yet Gabriele Greco of the Swedish University of Agricultural Sciences and colleagues suggest such structures might instead influence the propagation of web vibrations triggered by the impact of captured prey.
Greco and colleagues observed different stabilimentum geometries that were constructed by wasp spiders, Argiope bruennichi. The researchers then performed numerical simulations to explore how stabilimenta affect prey impact vibrations.
For waves generated at angles perpendicular to the threads spiralling out from the web centre, stabilimenta caused negligible delays in wave propagation.
However, for waves generated in the same direction as the spiral threads, vibrations in webs with stabilimenta propagated to a greater number of potential detection points across the web – where a spider might sense them – than in webs without stabilimenta.
This suggests that stabilimenta may boost a spider’s ability to pinpoint the location of unsuspecting prey caught in its web.
Female university students do much better in introductory physics exams if they have the option of retaking the tests. That’s according to a new analysis of almost two decades of US exam results for more than 26 000 students. The study’s authors say it shows that female students benefit from lower-stakes assessments – and that the persistent “gender grade gap” in physics exam results does not reflect a gender difference in physics knowledge or ability.
The study has been carried out by David Webb from the University of California, Davis, and Cassandra Paul from San Jose State University. It builds on previous work they did in 2023, which showed that the gender gap disappears in introductory physics classes that offer the chance for all students to retake the exams. That study did not, however, explore why the offer of a retake has such an impact.
In the new study, the duo analysed exam results from 1997 to 2015 for a series of introductory physics classes at a public university in the US. The dataset included 26 783 students, mostly in biosciences, of whom about 60% were female. Some of the classes let students retake exams while others did not, thereby letting the researchers explore why retakes close the gender gap.
When Webb and Paul examined the data for classes that offered retakes, they found that in first-attempt exams female students slightly outperformed their male counterparts. But male students performed better than female students in retakes.
This, the researchers argue, discounts the notion that retakes close the gender gap by allowing female students to improve their grades. Instead, they suggest that the benefit of retakes is that they lower the stakes of the first exam.
The team then compared the classes that offered retakes with those that did not, which they called high-stakes courses. They found that the gender gap in exam results was much larger in the high-stakes classes than the lower-stakes classes that allowed retakes.
“This suggests that high-stakes exams give a benefit to men, on average, [and] lowering the stakes of each exam can remove that bias ” Webb told Physics World. He thinks that as well as allowing students to retake exams, physics might benefit from not having comprehensive high-stakes final exams but instead “use final exam time to let students retake earlier exams”.
Earlier this year I met the Massachusetts-based steampunk artist Bruce Rosenbaum at the Global Physics Summit of the American Physical Society. He was exhibiting a beautiful sculpture of a “quantum engine” that was created in collaboration with physicists including NIST’s Nicole Yunger Halpern – who pioneered the scientific field of quantum steampunk.
I was so taken by the art and science of quantum steampunk that I promised Rosenbaum that I would chat with him and Yunger Halpern on the podcast – and here is that conversation. We begin by exploring the art of steampunk and how it is influenced by the technology of the 19th century. Then, we look at the physics of quantum steampunk, a field that weds modern concepts of quantum information with thermodynamics – which itself is a scientific triumph of the 19th century.
This podcast is supported by Atlas Technologies, specialists in custom aluminium and titanium vacuum chambers as well as bonded bimetal flanges and fittings used everywhere from physics labs to semiconductor fabs.
Progression of the Rayleigh–Taylor instability: Initially, an applied force (grey arrows) destabilizes the fluid interface between spin-up (blue) and spin-down (yellow) sodium atoms. The interface then develops nominally sinusoidal modulations where currents counterflowing in the two fluids (coloured arrows) induce vorticity at the interface (black symbols). The modulations subsequently acquire characteristic mushroom or spike shapes before dissolving into a turbulent mixture. (Courtesy: Taken from Science Advances11 35, 10.1126/sciadv.adw9752, licensed under CC BY-NC)
Researchers in the US have replicated a well-known fluid-dynamics process called the Rayleigh–Taylor instability on a quantum scale for the first time. The work opens the hydrodynamics of quantum gases to further exploration and could even create a new platform for understanding gravitational dynamics in the early universe.
If you’ve ever tried mixing oil with water, you’ll understand how the Rayleigh–Taylor instability (RTI) can develop. Due to their different molecular structures and the nature of the forces between their molecules, the two fluids do not mix well. After some time, they separate, forming a clear interface between oil and water.
Scientists have studied the dynamics of this interface upon perturbations – disturbances of the system – for nearly 150 years, with major work being done by the British physicists Lord Rayleigh in 1883 and Geoffrey Taylor in 1950. Under specific conditions related to the buoyant force of the fluid and the perturbative force causing the disturbance, they showed that this interface becomes unstable. Rather than simply oscillating, the system deviates from its initial state, leading to the formation of interesting geometric patterns such as mushroom clouds and filaments of gas in the Crab Nebula.
An interface of spins
To show that such dynamics occur not only in macroscopic structures, but also at a quantum scale, scientists at the University of Maryland and the Joint Quantum Institute (JQI) created a two-state quantum system using a Bose–Einstein condensate (BEC) of sodium (23Na) atoms. In this state of matter, the temperature is so low, the sodium atoms behave as a single coherent system, giving researchers precise control of their parameters.
The JQI team confine this BEC in a two-dimensional optical potential that essentially produces a 100 µm × 100 µm sheet of atoms in the horizontal plane. The scientists then apply a microwave pulse that excites half of the atoms from the spin-down to the spin-up state. By adding a small magnetic field gradient along one of the horizontal axes, they induce a force (the Stern–Gerlach force) that acts on the two spin components in opposite directions due to the differing signs of their magnetic moments. This creates a clear interface between the spin-up and the spin-down atoms.
Mushrooms and ripplons
To initiate the RTI, the scientists need to perturb this two-component BEC by reversing the magnetic field gradient, which consequently reverses the direction of the induced force. According to Ian Spielman, who led the work alongside co-principal investigator Gretchen Campbell, this wasn’t as easy as it sounds. “The most difficult part was preparing the initial state (horizontal interface) with high quality, and then reliably inverting the gradient rapidly and accurately,” Spielman says.
The researchers then investigated how the magnitude of this force difference, acting on the two sides of the interface, affected the dynamics of the two-component BEC. For a small differential force, they initially observed a sinusoidal modulation of the interface. After some time, the interface enters a nonlinear dynamics regime where the RTI manifests through the formation of mushroom clouds. Finally, it becomes a turbulent mixture. The larger the differential force, the more rapidly the system evolves.
Spin up and spin down: Experimental setup showing the vacuum chamber where the sodium atoms are prepared. (Courtesy: Spielman–Campbell laboratory, JQI)
While RTI dynamics like these were expected to occur in quantum fluids, Spielman points out that proving it required a BEC with the right internal interactions. The BEC of sodium atoms in their experimental setup is one such system.
In general, Spielman says that cold atoms are a great tool for studying RTI because the numerical techniques used to describe them do not suffer from the same flaws as the Navier–Stokes equation used to model classical fluid dynamics. However, he notes that the transition to turbulence is “a tough problem that resides at the boundary between two conceptually different ways of thinking”, pushing the capabilities of both analytical and numerical techniques.
The scientists were also able to excite waves known as ripplon modes that travel along the interface of the two-component BEC. These are equivalent to the classical capillary waves –“ripples” when a droplet impacts a water surface. Yanda Geng, a JQI PhD student working on this project, explains that every unstable RTI mode has a stable ripplon as a sibling. The difference is that ripplon modes only appear when a small sinusoidal modulation is added to the differential force. “Studying ripplon modes builds understanding of the underlying [RTI] mechanism,” Geng says.
The flow of the spins
In a further experiment, the team studied a phenomenon that occurs as the RTI progresses and the spin components of the BEC flow in opposite directions along part of their shared interface. This is known as an interfacial counterflow. By transferring half the atoms into the other spin state after initializing the RTI process, the scientists were able to generate a chain of quantum mechanical whirlpools – a vortex chain – along the interface in regions where interfacial counterflow occurred.
Spielman, Campbell and their team are now working to create a cleaner interface in their two-component BEC, which would allow a wider range of experiments. “We are considering the thermal properties of this interface as a 1D quantum ‘string’,” says Spielman, adding that the height of such an interface is, in effect, an ultra-sensitive thermometer. Spielman also notes that interfacial waves in higher dimensions (such as a 2D surface) could be used for simulations of gravitational physics.
Improving the efficiency of solar cells will likely be one of the key approaches to achieving net zero emissions in many parts of the world. Many types of solar cells will be required, with some of the better performances and efficiencies expected to come from multi-junction solar cells. Multi-junction solar cells comprise a vertical stack of semiconductor materials with distinct bandgaps, with each layer converting a different part of the solar spectrum to maximize conversion of the Sun’s energy to electricity.
When there are no constraints on the choice of materials, triple-junction solar cells can outperform double-junction and single-junction solar cells, with a power conversion efficiency (PCE) of up to 51% theoretically possible. But material constraints – due to fabrication complexity, cost or other technical challenges – mean that many such devices still perform far from the theoretical limits.
Perovskites are one of the most promising materials in the solar cell world today, but fabricating practical triple-junction solar cells beyond 1 cm2 in area has remained a challenge. A research team from Australia, China, Germany and Slovenia set out to change this, recently publishing a paper in Nature Nanotechnology describing the largest and most efficient triple-junction perovskite–perovskite–silicon tandem solar cell to date.
When asked why this device architecture was chosen, Anita Ho-Baillie, one of the lead authors from The University of Sydney, states: “I am interested in triple-junction cells because of the larger headroom for efficiency gains”.
Addressing surface defects in perovskite solar cells
Solar cells formed from metal halide perovskites have potential to be commercially viable, due to their cost-effectiveness, efficiency, ease of fabrication and their ability to be paired with silicon in multi-junction devices. The ease of fabrication means that the junctions can be directly fabricated on top of each other through monolithic integration – which leads to only two terminal connections, instead of four or six. However, these junctions can still contain surface defects.
To enhance the performance and resilience of their triple-junction cell (top and middle perovskite junctions on a bottom silicon cell), the researchers optimized the chemistry of the perovskite material and the cell design. They addressed surface defects in the top perovskite junction by replacing traditional lithium fluoride materials with piperazine-1,4-diium chloride (PDCl). They also replaced methylammonium – which is commonly used in perovskite cells – with rubidium. “The rubidium incorporation in the bulk and the PDCl surface treatment improved the light stability of the cell,” explains Ho-Baillie.
To connect the two perovskite junctions, the team used gold nanoparticles on tin oxide. Because the gold was in a nanoparticle form, the junctions could be engineered to maximize the flow of electric charge and light absorption by the solar cell.
“Another interesting aspect of the study is the visualization of the gold nanoparticles [using transmission electron microscopy] and the critical point when they become a semi-continuous film, which is detrimental to the multi-junction cell performance due to its parasitic absorption,” says Ho-Baillie. “The optimization for achieving minimal particle coverage while achieving sufficient ohmic contact for vertical carrier flow are useful insights”.
Record performance for a large-scale perovskite triple-junction cell
Using these design strategies, Ho-Baillie and colleagues developed a 16 cm2 triple-junction cell that achieved an independently certified steady-state PCE of 23.3% – the highest reported for a large-area device. While triple-junction perovskite solar cells have exhibited higher PCEs – with all-perovskite triple-junction cells reaching 28.7% and perovskite–perovskite–silicon devices reaching 27.1% – these were all achieved on a 1 cm2 cell, not a large-area cell.
In this study, the researchers also developed a 1 cm2 cell that was close to the best, with a PCE of 27.06%, but it is the large-area cell that’s the record breaker. The 1 cm2 cell also passed the International Electrotechnical Commission’s (IEC) 61215 thermal cycling test, which exposes the cell to 200 cycles under extreme temperature swings, ranging from –40 to 85°C. During this test, the 1 cm2 cell retained 95% of its initial efficiency after 407 h of continuous operation.
The combination of the successful thermal cycling test combined with the high efficiencies on a larger cell shows that there could be potential for this triple-junction architecture in real-world settings in the near future, even though they are still far away from their theoretical limits.
It’s rare to come across someone who’s been responsible for enabling a seismic shift in society that has affected almost everyone and everything. Tim Berners-Lee, who invented the World Wide Web, is one such person. His new memoir This is for Everyone unfolds the history and development of the Web and, in places, of the man himself.
Berners-Lee was born in London in 1955 to parents, originally from Birmingham, who met while working on the Ferranti Mark 1 computer and knew Alan Turing. Theirs was a creative, intellectual and slightly chaotic household. His mother could maintain a motorbike with fence wire and pliers, and was a crusader for equal rights in the workplace. His father – brilliant and absent minded – taught Berners-Lee about computers and queuing theory. A childhood of camping and model trains, it was, in Berners-Lee’s view, idyllic.
Berners-Lee had the good fortune to be supported by a series of teachers and managers who recognized his potential and unique way of working. He studied physics at the University of Oxford (his tutor “going with the flow” of Berners-Lee’s unconventional notation and ability to approach problems from oblique angles) and built his own computer. After graduating, he married and, following a couple of jobs, took a six-month placement at the CERN particle-physics lab in Geneva in 1985.
This placement set “a seed that sprouted into a tool that shook up the world”. Berners-Lee saw how difficult it was to share information stored in different languages in incompatible computer systems and how, in contrast, information flowed easily when researchers met over coffee, connected semi-randomly and talked. While at CERN, he therefore wrote a rough prototype for a program to link information in a type of web rather than a structured hierarchy.
Back at CERN, Tim Berners-Lee developed his vision of a “universal portal” to information
The placement ended and the program was ignored, but four years later Berners-Lee was back at CERN. Now divorced and soon to remarry, he developed his vision of a “universal portal” to information. It proved to be the perfect time. All the tools necessary to achieve the Web – the Internet, address labelling of computers, network cables, data protocols, the hypertext language that allowed cross-referencing of text and links on the same computer – had already been developed by others.
Berners-Lee saw the need for a user-friendly interface, using hypertext that could link to information on other computers across the world. His excitement was “uncontainable”, and according to his line manager “few of us if any could understand what he was talking about”. But Berners-Lee’s managers supported him and freed his time away from his actual job to become the world’s first web developer.
Having a vision was one thing, but getting others to share it was another. People at CERN only really started to use the Web properly once the lab’s internal phone book was made available on it. As a student at the time, I can confirm that it was much, much easier to use the Web than log on to CERN’s clunky IBM mainframe, where phone numbers had previously been stored.
Wider adoption relied on a set of volunteer developers, working with open-source software, to make browsers and platforms that were attractive and easy to use. CERN agreed to donate the intellectual property for web software to the public domain, which helped. But the path to today’s Web was not smooth: standards risked diverging and companies wanted to build applications that hindered information sharing.
Feeling the “the Web was outgrowing my institution” and “would be a distraction” to a lab whose core mission was physics, Berners-Lee moved to the Massachusetts Institute of Technology in 1994. There he founded the World Wide Web Consortium (W3C) to ensure consistent, accessible standards were followed by everyone as the Web developed into a global enterprise. The progression sounds straightforward although earlier accounts, such as James Gillies and Robert Caillau’s 2000 book How the Web Was Born, imply some rivalry between institutions that is glossed over here.
Initially inclined to advise people to share good things and not search for bad things, Berners-Lee had reckoned without the insidious power of “manipulative and coercive” algorithms on social networks
The rest is history, but not quite the history that Berners-Lee had in mind. By 1995 big business had discovered the possibilities of the Web to maximize influence and profit. Initially inclined to advise people to share good things and not search for bad things, Berners-Lee had reckoned without the insidious power of “manipulative and coercive” algorithms on social networks. Collaborative sites like Wikipedia are closer to his vision of an ideal Web; an emergent good arising from individual empowerment. The flip side of human nature seems to come as a surprise.
The rest of the book brings us up to date with Berners-Lee’s concerns (data, privacy, misuse of AI, toxic online culture), his hopes (the good use of AI), a third marriage and his move into a data-handling business. There are some big awards and an impressive amount of name dropping; he is excited by Order of Merit lunches with the Queen and by sitting next to Paul McCartney’s family at the opening ceremony to the London Olympics in 2012. A flick through the index reveals names ranging from Al Gore and Bono to Lucien Freud. These are not your average computing technology circles.
There are brief character studies to illustrate some of the main players, but don’t expect much insight into their lives. This goes for Berners-Lee too, who doesn’t step back to particularly reflect on those around him, or indeed his own motives beyond that vision of a Web for all enabling the best of humankind. He is firmly future focused.
Still, there is no-one more qualified to describe what the Web was intended for, its core philosophy, and what caused it to develop to where it is today. You’ll enjoy the book whether you want an insight into the inner workings that make your web browsing possible, relive old and forgotten browser names, or see how big tech wants to monetize and monopolize your online time. It is an easy read from an important voice.
The book ends with a passionate statement for what the future could be, with businesses and individuals working together to switch the Web from “the attention economy to the intention economy”. It’s a future where users are no longer distracted by social media and manipulated by attention-grabbing algorithms; instead, computers and services do what users want them to do, with the information that users want them to have.
Berners-Lee is still optimistic, still an incurable idealist, still driven by vision. And perhaps still a little naïve too in believing that everyone’s values will align this time.
From immeasurable to measurable Microwave pulses and lattice depth control manipulate fermions on a lattice (left), converting a hard-to-detect signal into a brickwork pattern (right) that reveals d-wave pairing, a key signature of high-temperature superconductors. (Courtesy: Adapted from D K Mark et al. Phys. Rev. Lett.135 123402 (2025))
Understanding the mechanism of high-temperature superconductivity could unlock powerful technologies, from efficient energy transmission to medical imaging, supercomputing and more. Researchers at Harvard University and the Massachusetts Institute of Technology have designed a new protocol to study a candidate model for high-temperature superconductivity (HTS), described in Physical Review Letters.
The model, known as the Fermi-Hubbard model, is believed to capture the essential physics of cuprate high-temperature superconductors, materials composed of copper and oxygen. The model describes fermions, such as electrons, moving on a lattice. The fermions experience two competing effects: tunnelling and on-site interaction. Imagine students in a classroom: they may expend energy to switch seats (tunnelling), avoid a crowded desk (repulsive on-site interaction) or share desks with friends (attractive on-site interaction). Such behaviour mirrors that of electrons moving between lattice sites.
Daniel Mark, first author of the study, notes that: “After nearly four decades of research, there are many detailed numerical studies and theoretical models on how superconductivity can emerge from the Fermi-Hubbard model, but there is no clear consensus [on exactly how it emerges].”
A precursor to understanding the underlying mechanism is testing whether the Fermi-Hubbard model gives rise to an important signature of cuprate HTS: d-wave pairing. This is a special type of electron pairing where the strength and sign of the pairing depend on the direction of electron motion. It contrasts with conventional low-temperature superconductors that exhibit s-wave pairing, in which the pairing strength is uniform in all directions.
Although physicists have developed robust methods for simulating the Fermi-Hubbard model with ultracold atoms, measuring d-wave pairing has been notoriously difficult. The new protocol aims to change that.
A change of perspective
A key ingredient in the protocol is the team’s use of “repulsive-to-attractive mapping”. The physics of HTS is often described by the repulsive Fermi-Hubbard model, in which electrons pay an energetic penalty for occupying the same lattice site, like disagreeing students sharing a desk. In this model, detecting d-wave pairing requires fermions to maintain a fragile quantum state as they move over large distances, which necessitates carefully fine-tuned experimental parameters.
To make the measurement more robust to experimental imperfection, the authors use a clever mathematical trick: they map from the repulsive model to the attractive one. In the attractive model, electrons receive an energetic benefit from being close together, like two friends in a classroom. The mapping is achieved by a particle–hole transformation, wherein spin-down electrons are reinterpreted as holes and vice versa. After mapping, the d-wave pairing signal becomes an observable that conserves local fermion number, thereby circumventing the challenge of long-range motion.
Pulse sequence Carefully timed pulses, including microwave, hopping and idling pulses transform the state of the system for easier readout. (Courtesy: D K Mark et al. Phys. Rev. Lett.135 123402 (2025))
In its initial form, the d-wave pairing signal is difficult to measure. Drawing inspiration from digital quantum gates, the researchers divide their complex system into subsystems composed of pairs of lattice sites or dimers. Then, they apply a pulse sequence to make the observable measurable by simply counting fermions – a standard technique in the lab.
The pulse sequence begins with a global microwave pulse to manipulate the spin of the fermions, followed by a series of “hopping” and “idling” steps. The hopping step involves lowering the barrier between lattice sites, thereby increasing tunnelling. The idling step involves raising the barrier, allowing the system to evolve without tunnelling. Every step is carefully timed to reveal the d-wave pairing information at the end of the sequence.
The researchers report that their protocol is sample-efficient, experimentally viable, and generalizable to other observables that conserve local fermion number and act on dimers.
This work adds to a growing field that combines components of analogue quantum systems with digital gates to deeply study complex quantum phenomena. “All the experimental ingredients in our protocol have been demonstrated in existing experiments, and we are in discussion with several groups on possible use cases,” Mark tells Physics World.